Abstract
Objectives: Health Promotion Units within New South Wales (NSW) local health districts (LHDs) frequently collaborate and test innovations to address priority health issues or approaches to support the implementation of a health promotion program in a way that is consistent with the needs, resources, and contexts of their regions. Compatible with learning health system approaches, mechanisms to facilitate the exchange of evidence and expertise across districts could improve the collective impact of health promotion services across the state. This study aimed to assess the use of a health promotion Community of Practice (CoP) model as a strategy to achieve this.
Type of program or service: This paper describes and shares experiences from the development and piloting process of a CoP model to develop, evaluate and exchange learnings to improve approaches to support the adoption of an effective healthy lunchbox program (‘SWAP IT’) across three LHDs.
Results: The functioning of the CoP was supported by key activities, funding and infrastructure over a 2-year period, including: planning workshops, implementation check-ins, and knowledge exchange meetings. A particularly novel aspect of the CoP was the harmonised evaluation of different, locally developed strategies to facilitate program adoption across the three LHDs. The alignment of the CoP with local and state priorities, as well as the operation of the CoP in a way that did not impose significant time demands, was seen as important for the sustainability of the CoP.
Lessons learnt: Findings from the piloting process suggest that a formalised CoP shows promise as an effective model to enhance health promotion collaboration, information sharing and practice across LHDs, which may be suitable for broader application across the state.
Full text
Introduction
Local health district (LHD) Health Promotion Units within New South Wales (NSW), Australia, are responsible for providing health promotion services to their community. While these units respond to local community needs, the focus of their work is largely guided by priorities set by the NSW Ministry of Health (MOH). In some cases, this includes the delivery of specific state-wide programs for which each LHD has a funding agreement and performance target.
Health Promotion Units frequently develop and test innovations to improve health promotion services in a way that is consistent with the needs, resources, and contexts of the regions they serve. While such learnings (and innovation) are intended for local service improvement, they are likely to be of considerable value to other LHDs seeking to address the same health issue. Mechanisms to facilitate the collaboration and exchange of evidence, experience and expertise across districts, such as networks, are often established by MOH around topic areas. Networks, however, provide an opportunity for practice information exchange rather than the coordinated creation of new knowledge for the purpose of improvement.1
‘Learning health systems’ use service, patient and/or population data to address and continually improve the impact of preventive (and other services).2 Data-driven Communities of Practice (CoP) have been recommended as one structure to support rapid improvement in health practice consistent with learning health system approaches to prevention.3 Communities of Practice are defined by Wenger-Trayner as “groups of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly”.4 The purpose of a CoP is to share best practices and create new knowledge to advance a domain of practice. They represent structures requiring greater engagement by participants than networks, underpinned by an intentional commitment of members to collectively advance practice and share knowledge and resources.4 CoPs have three prevailing characteristics: domain (members have a shared domain of interest, competence and commitment); community (members pursue this interest through joint discussion, information sharing and relationship building); and practice (members are actual practitioners in the domain of interest and develop a shared repertoire of resources). CoPs can also provide structures to coordinate and embed evaluations in practice to achieve the stated improvement goals and facilitate problem-solving, reflective practice and networking.5
Given the potential for a CoP to efficiently improve health promotion practice, the Health Promotion Units of three NSW LHDs sought to form a CoP model to develop, evaluate and exchange learnings to strengthen approaches to support the adoption of an effective healthy school lunchbox program (‘SWAP IT’) by primary schools across three LHDs. This paper describes and shares the experiences relating to the development and piloting process of the CoP model.
Purpose of the Community of Practice (CoP) model
The SWAP IT program was first piloted within the Hunter New England LHD to address concerns that existing state-wide school-based health promotion programs traditionally focused on school canteens and did not include sufficient strategies to improve the nutritional quality of foods packed in student lunchboxes brought from home.
Following the pilot, a randomised controlled trial was conducted collaboratively across three geographically close LHDs, with findings demonstrating the effectiveness of SWAP IT on child health outcomes.6-8 This process resulted in the LHDs being engaged with SWAP IT and experienced with the program resources and implementation. Following the trial, health promotion practitioners from the LHDs expressed interest in providing SWAP IT to all primary schools within their regions. To facilitate this process, a working group was established with health promotion practitioners from the three LHDs in November 2020 to maximise the adoption (or scale-up) of the SWAP IT program. Following the drafting of the Terms of Reference for the group, it was identified that the purpose and activities of the group strongly aligned with the characteristics of a CoP – and, as such, is now referred to as the SWAP IT CoP. The key characteristics of a CoP and how they have been employed within the SWAP IT CoP are described in Figure 1.
Figure 1. Characteristics of the SWAP IT Community of Practice (click figure to enlarge)

CoP = Community of Practice; KPIs = key performance indicators; LHDs = local health districts; MoH = Ministry of Health
Coordination and support
A Terms of Reference document was collaboratively drafted with contributions from all participating LHDs to outline the following: i) the purpose and aims of the group; ii) roles and responsibilities of participants; and iii) key activities and functions of the group. The purpose and aims detailed within the Terms of Reference reflected the underlying goal of the group, that is, to improve health promotion practice and foster great collaboration, engagement and partnerships between LHDs in health promotion innovation, evaluation and learnings for collective benefit.
Broadly, health promotion staff within each LHD were responsible for: undertaking the scale-up of SWAP IT within their regions, tailored to align with their service plans, resources and staffing; participating in and engaging with the activities of the CoP; and contributing to the sharing and exchange of learnings to improve approaches to maximise school adoption of the SWAP IT program. Additionally, the National Centre of Implementation Science (NCOIS), a collaborating research centre of which the three LHDs are research and translation partners9, provided funding for staffing, infrastructure and coordination support for the CoP, including the facilitation of workshops, implementation check-ins, knowledge exchange meetings, evaluation of the CoP and additional support on request.
Organising framework and activities
The functioning of the SWAP IT CoP was supported by key activities and infrastructure over a 2-year period, as described in Figure 2.
Figure 2. Key activities of the SWAP IT CoP (click figure to enlarge)
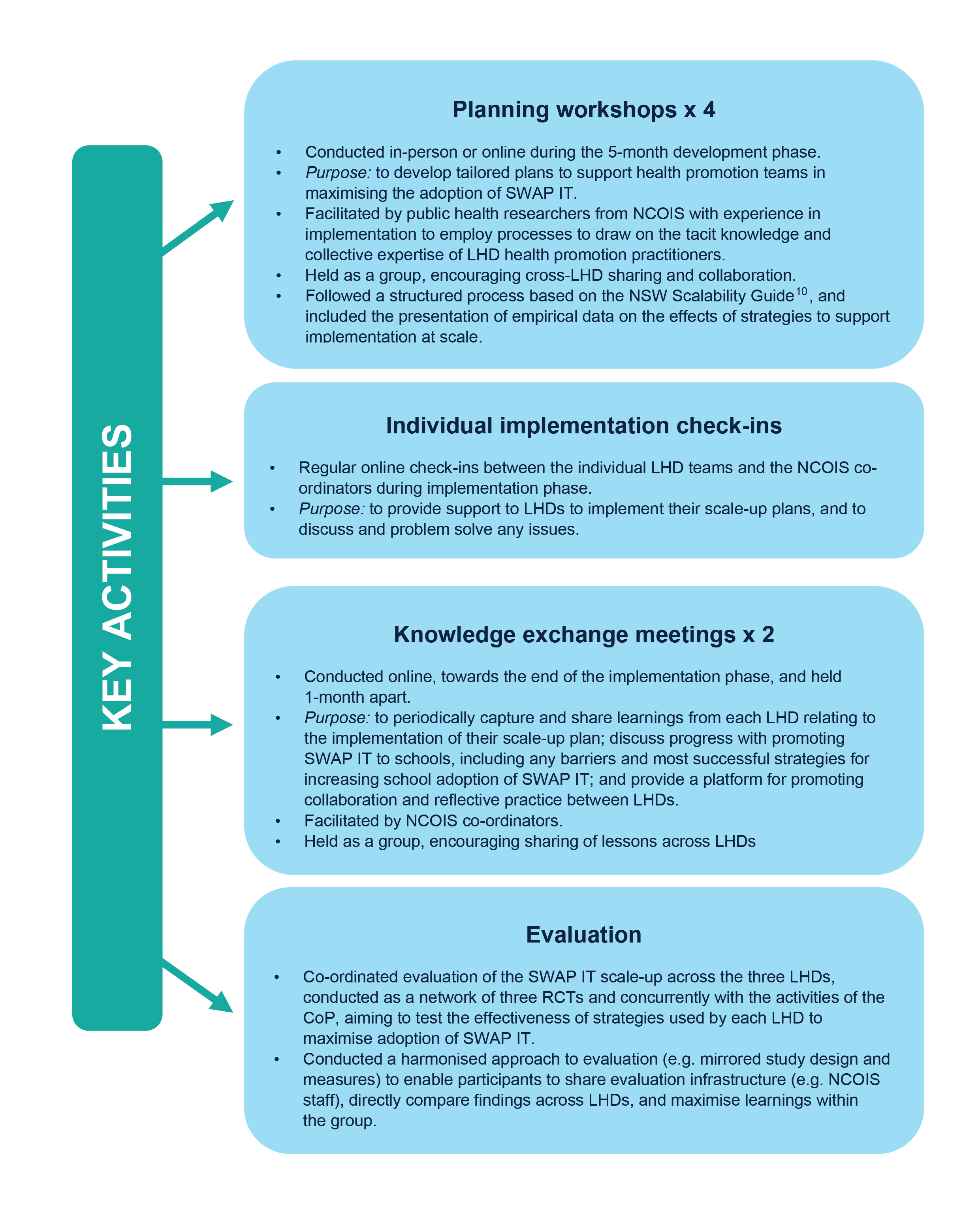
CoP = Community of Practice; LHD = local health district; NCOIS = National Centre of Implementation Science; RCT = randomised controlled trial
Additional technology infrastructure was developed to provide a mechanism for knowledge and resource sharing among CoP members. For example, a Microsoft Teams channel was established to facilitate sharing of resources, recruitment and promotional materials across the LHDs. Additionally, a website was developed to enable school registration of SWAP IT. School registration data captured via the website is automatically disseminated to LHDs, providing continual feedback regarding the success of their scale-up plans.
Key learnings and implications for future practice
The process of developing and piloting a CoP to maximise the adoption of SWAP IT has resulted in several learnings for the sustainability of the CoP and the potential application of a similar approach more broadly across NSW. Here, we share these learnings from the perspectives of the LHD and NCOIS staff that were engaged in the CoP, organised by the key characteristics of CoPs defined by Wegner-Trayner4 and outlined in Figure 1. These learnings and insights were captured during knowledge exchange meetings held with LHD health promotion staff throughout the process of developing and piloting the model.
Domain
Overall, health promotion staff across the three LHDs had a shared interest and commitment towards maximising the adoption of the SWAP IT program within schools in their regions. This commitment was supported by district health promotion directors and funding from NCOIS to enable the use of health service infrastructure to scale up the program. However, due to unavoidable staffing reallocations and shifting priorities of the health service and other key partners, such as the education sector as a result of the coronavirus disease 2019 (COVID-19) pandemic (e.g. staff being reallocated to contact tracing), the perceived priority of maximising the adoption of SWAP IT, and thus the SWAP IT CoP, wavered. Additionally, traditional approaches employed by LHDs to encourage the uptake of health promotion programs in schools were limited due to the impacts of the COVID-19 pandemic.
As such, the benefits and success of the CoP and its sustainability are perceived to be highly dependent on the alignment of the CoP with the priorities of the health service at a state (i.e. NSW MOH) and LHD-level. The SWAP IT CoP was established to scale up an evidence-based lunchbox program, an identified gap in current NSW MOH school-based nutrition programs. However, it was felt continuation and/or expansion of the CoP is reliant on the CoP program of interest not only being a priority for LHDs, but also NSW MOH and other key sectors (e.g. Department of Education).
Community
Health promotion staff across the three LHDs participated in joint discussions, information sharing and relationship building to maximise the adoption of SWAP IT. The support, capacity building and resource support provided by the NCOIS coordinators, including the regular implementation check-ins, was a core component of the CoP. Health promotion staff perceived as useful in supporting them to implement their scale-up plans and maximise adoption of SWAP IT in their regions. Additionally, health promotion staff saw the establishment of a dedicated Microsoft Teams channel as practical infrastructure to support information sharing. Overall, this approach improved collaboration across LHDs and led to productive exchanges to yield changes in practice. For example, health promotion staff shared learnings on navigating the impact of COVID-19 school disruptions on the delivery of usual school-based health promotion activities and the execution of their scale-up plans. As a result of sharing these learnings, other LHDs adjusted their timelines and approach to executing their scale-up strategies in their regions to maximise the adoption of SWAP IT. Additionally, emails one health promotion team developed with embedded videos targeting school barriers to adopting SWAP IT were shared and incorporated within other LHDs scale-up plans.
Operation of the CoP in a productive way but did not impose significant time demands on an already stretched health promotion workforce, which recognised the variation in structure and resources across LHDs, was seen as particularly important. For example, the capacity of the health promotion workforce and available resources to support and engage with activities of the CoP (e.g. knowledge exchange meetings) may vary greatly across LHDs. As such, the CoP model sustainability relies on its activities being consistent with existing LHD capacity and infrastructure. Acknowledging this, the community component of the CoP could potentially be integrated with existing networks and infrastructure currently available to LHD health promotion units. Broader cross-LHD networks and support (e.g. SharePoint site to facilitate resource sharing) exist and provide a platform to collaborate with other LHDs on various health promotion programs. Similarly, the Group for Research, Evaluation and Translation in Health Promotion (‘GREAT-HP’) recenty established by NCOIS researchers – which also has NCOIS coordination and support to build LHD research capacity and knowledge translation for the NSW Health Promotion workforce – may provide a vehicle to embed a CoP and scale-up effective health promotion programs (such as SWAP IT). Exploring these and other opportunities appears warranted.
Practice
The three LHDs participating in the SWAP IT CoP employed staff to support the implementation of school-based health promotion programs, with all staff in the CoP being experienced in health promotion and implementing SWAP IT. This familiarity with SWAP IT was perceived as useful when communicating with schools and encouraging them to adopt the program. Unlike collaborative research partnerships requiring an intervention or implementation strategy to be executed in the same way across participating sites (or LHDs) to ensure fidelity, the systems being tested to support SWAP IT adoption were developed by LHDs to be consistent with local context and capacities. This was seen as beneficial to maximise the relevance of evaluation findings for local decision making. The harmonised (use of the same measures) evaluation was also undertaken centrally with shared infrastructure, representing an efficient use of evaluation resources and expertise and supporting learning.
Nonetheless, further evaluation is recommended as part of a CoP to determine if it has successfully improved both individual and group (i.e. LHD) outcomes, is serving its intended purpose and is still relevant to the needs and priorities of the group.5 The harmonised SWAP IT evaluation findings on adoption outcomes will be reported separately. However, changes in health promotion capacity, practice, collaborations and practitioner knowledge of preventive health systems or performance outcomes also warrant formal evaluation.
Conclusions
The development of a CoP shows promise as an effective approach to improving health promotion practice across NSW LHDs and has the potential to address limitations of other health promotion collaboration approaches that are less data-driven, such as discussion groups and networks. The CoP also demonstrates the feasibility of collective action, data sharing and knowledge exchange across LHDs consistent with recommended learning health system approaches for prevention.11 In order for a NSW LHD health promotion CoP to be effective and sustainable, dedicated resources to support the CoP coordination is required, and the health promotion program/s of interest must closely align with the priorities of the LHDs, their communities and NSW MOH. Additionally, integrating the CoP activities within existing networks or leveraging existing infrastructure should be considered to enhance sustainability further.
†NCOIS Research Collaborative, NSW, Australia
The NCOIS (National Centre of Implementation Science) Research Collaborative (consortium authorship) includes:
Lisa Janssen, School of Medicine and Public Health, University of Newcastle, and NCOIS
Nicola Kerr, Mid North Coast Local Health District (MNCLHD)
Nicole J Kajons, Central Coast Local Health District (CCLHD)
Justine Gowland-Ella, CCLHD
Katie Robinson, Hunter New England Local Health District (HNELHD)
Jannah Jones, HNELHD, School of Medicine and Health, University of Newcastle, Hunter Medical Research Institute (HMRI), NCOIS
Karen Gilham, HNELHD
Alison Brown, HNELHD, School of Medicine and Public Health, University of Newcastle, HMRI, NCOIS.
Acknowledgements
The NCOIS is a National Health and Medical Research Centre Centre for Research Excellence (APP1153479) that provided funding to each local health district to support the implementation of their scale-up plans. CB receives salary support from a NSW Ministry of Health PRSP Research Fellowship. LW is supported by an NHMRC Investigator Grant (APP11960419) and NSW Cardiovascular Research Capacity Program (H20/28248). RS is supported by a Medical Research Future Fund Fellowship (APP1150661) and a Hunter New England Clinical Research Fellowship. The contents of this manuscript are the responsibility of authors and do not reflect the views of NSW Ministry of Health or NHMRC.
The authors would like to acknowledge all health promotion staff from the three participating LHDs involved in the scale-up of SWAP IT within their regions.
Peer review and provenance
Externally peer reviewed, not commissioned.

© 2023 Barnes et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Cunningham FC, Ranmuthugala G, Plumb J, Georgiou A, Westbrook JI, Braithwaite J. Health professional networks as a vector for improving healthcare quality and safety: a systematic review. BMJ Qual Saf. 2012;21(3):239–49. CrossRef | PubMed
- 2. Oh A, Abazeed A, Chambers DA. Policy implementation science to advance population health: the potential for learning health policy systems. Front Public Health. 2021;9:681602. CrossRef | PubMed
- 3. Penney LS, Homoya BJ, Damush TM, Rattray NA, Miech EJ, Myers LJ, et al. Seeding structures for a community of practice focused on transient ischemic attack (TIA): implementing across disciplines and waves. J Gen Intern Med. 2021;36(2):313–21. CrossRef | PubMed
- 4. Wenger-Trayner E, Wenger-Trayner B. An introduction to communities of practice: a brief overview of the concept and its uses. Portugal: Wegner-Trayner; 2015 [cited 2022 Oct 18]. Available from: www.wenger-trayner.com/introduction-to-communities-of-practice
- 5. Barbour L, Armstrong R, Condron P, Palermo C. Communities of practice to improve public health outcomes: a systematic review. Journal of Knowledge Management. 2018;22(2);326–343. CrossRef
- 6. Barnes C, Hall A, Nathan N, Sutherland R, McCarthy N, Pettet M, et al. Efficacy of a school-based physical activity and nutrition intervention on child weight status: Findings from a cluster randomized controlled trial. Prev Med. 2021;153:106822. CrossRef | PubMed
- 7. Sutherland R, Brown A, Nathan N, Yoong S, Janssen L, Chooi A, et al. A multicomponent mHealth-based intervention (SWAP IT) to decrease the consumption of discretionary foods packed in school lunchboxes: type I effectiveness – implementation hybrid cluster randomized controlled trial. J Med Internet Res. 2021;23(6):e25256. CrossRef | PubMed
- 8. Sutherland R, Nathan N, Brown A, Yoong S, Finch M, Lecathelinais C, et al. A randomized controlled trial to assess the potential efficacy, feasibility and acceptability of an m-health intervention targeting parents of school aged children to improve the nutritional quality of foods packed in the lunchbox ‘SWAP IT’. Int J Behav Nutr Phys Act.. 2019;16(1):54. CrossRef | PubMed
- 9. National Centre of Implementation Science. About Us. Newcastle; NCOIS; 2022 [cited 2022 Oct 18]. Available from: ncois.org.au/
- 10. NSW Government. Centre for Epidemiology and Evidence. Increasing the scale of population health interventions: a guide. Sydney: NSW Ministry of Health; 2014 [cited 2023 Aug 1]. Available from: https://www.health.nsw.gov.au/research/Publications/scalability-guide.pdf
- 11. Wolfenden L, Hawe P, Rychetnik L, Sutherland R, Barnes C, Yoong S, et al. A call to action: more collaborative implementation research is needed to prevent chronic disease. Aust N Z J Public Health. 2022;46(5):549–53. CrossRef | PubMed