Abstract
Objectives and importance of study: Despite the abundance of mental health research during the pandemic, there is limited evidence exploring mental health presentations to Australian general practice. This study examined the utilisation of telehealth for mental health consultations in Australian general practice during the COVID-19 pandemic. The objectives were to: 1) determine the proportion of mental health services delivered via telehealth between March 2020 and November 2021; 2) determine the types of mental health consultations most frequently delivered via telehealth; and 3) model the sociodemographic characteristics of patients using telehealth mental health consultations, including consultation type.
Study type: Retrospective observational study.
Methods: We used Medicare Benefits Schedule service item numbers to distinguish mental health consultations in de-identified electronic general practice data. We stratified the proportions of face-to-face, video, and telephone mental health consultations by state and consultation type. We used two mixed-effects logistic models to assess the variation in the likelihood of i) a telehealth (video/telephone) compared to a face-to-face consultation and ii) a video compared to telephone consultation; by sociodemographic characteristics.
Results: The study comprised 874 249 mental health consultations. Telehealth use peaked in Victoria (61.6%) during July 2020 and in NSW during August 2021 (52.5%). Telehealth use continued throughout 2021 with an increase in video consultations from July 2021 onwards in both states. Proportions of mental health treatment plan consultations via telephone decreased from July 2021 with a concomitant increase in video. Telehealth was more likely to be used by females, in Victoria, in regional/remote regions and during 2020. Video was more likely to be used than telephone for mental health treatment plans/reviews compared with mental health consultations. Compared with people aged 25–29, video was most likely to be used by ages 20–24 and least by those aged 80 and over. There was no evidence for sex differences when comparing telephone and video.
Conclusions: This study presents a comprehensive understanding of the important role telehealth played in the delivery of mental health consultations during the first 21 months of the pandemic, including sociodemographics of patients utilising telehealth. The findings can assist general practices with future planning for the delivery of mental health services via telehealth.
Full text
Introduction
As the coronavirus disease 2019 (COVID-19) pandemic continues, countries around the world continue to experience waves of infections. In Australia, case numbers in 2021 were higher than those of the previous year, and confirmed cases during the first 6 months of 2022 far exceeded those of 2020 and 2021 combined.1 Between March and early May 2020, cross-sectional online surveys in Australia gauged the impact of the COVID-19 outbreak on the mental health (MH) of Australian adults.2-6 The prevalence of self-reported clinically significant symptoms of depression and anxiety2,5, high levels of negative emotions6 and a decline in mental health3,4 were common findings during the first 3 months of the pandemic. The Australian Institute of Health and Welfare (AIHW) has reported the ongoing MH impact of COVID-19 through weekly service activity graphs including online MH support/crisis services, Medicare Benefits Schedule (MBS) (government subsidised consultations) and Pharmaceutical Benefits Scheme (government subsidised medicines) activity.7
Despite the abundance of MH research during the pandemic, there is limited evidence exploring MH presentations to Australian general practice8,9, even though general practitioners (GPs) provided 29% of MH-specific MBS services during 2020–2021.10 As primary care providers, GPs have an important role in the diagnosis, treatment and/or referral of patients presenting with MH concerns. In March 2020, the Australian Government implemented measures to increase the availability of MH services across Australia. This included the introduction of temporary MBS items for general practice MH-telehealth consultations, provided via either telephone or video modalities.11 Nationally, the provision of MH services via telehealth for all MH service providers reached just over 50% of all MBS mental health services, in April 2020.7 Analysis of general practice activity during the first 4 weeks of the pandemic showed that telehealth (telephone and video combined) exceeded face-to-face MH consultations between weeks 30 and 37.12
There is limited understanding of telehealth use for MH consultations in general practice beyond the first year of the pandemic. The gaps in knowledge include which types of patients chose to use telehealth for MH services, and whether usage was sustained over time. Changes introduced to MBS telehealth service items in July 2021 reduced the number of subsidised MH services available via telephone (see Supplementary File 1, available from: doi.org/10.25949/23826831.v1), and the government announced in December 2021 that telehealth would “become a permanent feature of primary health care”.13 There is a need to understand MH-telehealth patient demographics to help general practices plan infrastructure for the future provision of MH-telehealth services. This study aimed to quantify the use of telehealth for MH consultations during the COVID-19 pandemic in general practice, in the Australian states of New South Wales (NSW) and Victoria, over a period of 21 months from the start of the pandemic. The objectives were to:
- Determine the proportion of MH services delivered via telehealth (telephone and video) between March 2020 and November 2021
- Determine the types of MH consultations most frequently delivered via telehealth
- Model the sociodemographic characteristics of patients who utilised telehealth for MH consultations, including MH consultation type.
Methods
Australian context
During the study period (March 2020 to 30 November 2021), Australian states and territories experienced three main waves of COVID-19.14 The first wave was from March to May 2020, the second wave was between June and November 2020 (predominantly impacting Victoria) and the third Delta wave was between July and December 2021. The Delta wave was the most significant until the Omicron variant was detected in Australia during the last week of the study period. General practice involvement in the Australian COVID-19 vaccination program began in March 2021.15
Data source and study population
De-identified electronic health record data from 715 general practices (296 from NSW; 419 from Victoria) between March 2020 and 30 November 2021 were extracted retrospectively by the data custodians, Outcome Health, using their Population Level Analysis and Reporting (POLAR) extraction tool. POLAR is a platform developed and maintained by Outcome Health to provide data analytic services to primary health networks and general practices, including de-identified data for research16 Details of POLAR have been published previously.17 The study population was derived using all available MBS records and patient sociodemographic records in the extracted data. Sociodemographic characteristics of patients were linked to MBS records using a non-identifiable patient ID with a 1:many relationship.
Data variables
MBS item claims (billing data) were used to distinguish and determine consultation types. MH consultations were defined as MBS item numbers for MH-specific consultations, including eating disorders and consultations for residential aged care patients (see Supplementary File 1, available from: doi.org/10.25949/23826831.v1). We included MH services provided by vocationally and non-vocationally recognised doctors (defined in Supplementary File 1) working in general practice in the analysis. We excluded MBS items for allied health professionals (e.g. psychologists) working in general practice. We used postcodes to determine socioeconomic status (SES) based on the Australian Bureau of Statistics (ABS) Socioeconomic Indexes for Areas (SEIFA).18 We also used postcode to determine remoteness of the patient’s residence, based on the ABS Australian Statistical Geography Standard (ASGS) Remoteness structure19 with major cities designated as metropolitan and regional and remote areas designated as regional/remote.
Statistical methods
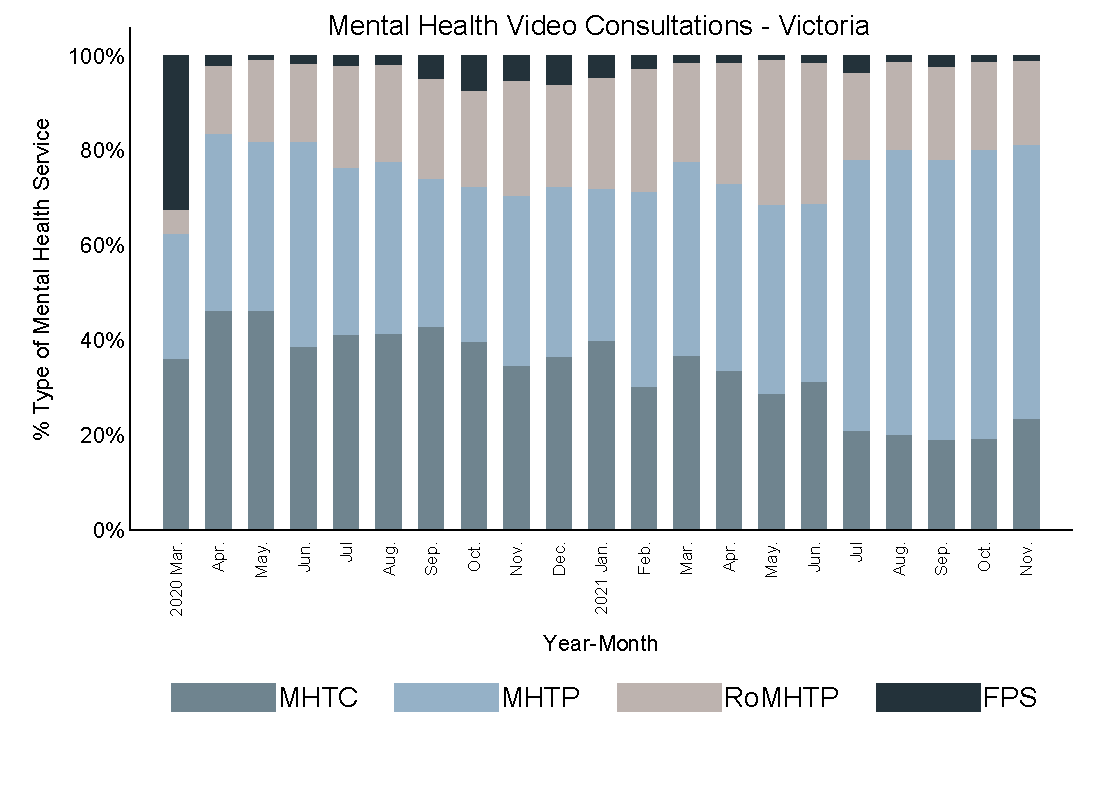
We determined monthly numbers of face-to-face, video and telephone MH consultations for all MH consultations (objective 1) and by MH consultation type (objective 2). These were then divided by the denominator, the total MH consultations overall (objective 1) and by MH consultation type (objective 2) for the respective month. We stratified the analysis by state, presented separately as percentage stacked bar charts. We grouped MBS items into four consultation types: MH treatment consultations (MHTC), MH treatment plans (MHTP), reviews of MH treatment plans (RoMHTP) and focused psychological strategies (FPS), as detailed in Supplementary File 2 (available from: doi.org/10.25949/23826831.v1)
We formed two mixed-effects logistic models to address objective 3. The first model assessed the variation in the likelihood of a telehealth (video or telephone) compared to a face-to-face consultation by sociodemographic characteristics. The rationale for the model was to assess sociodemographic factors which may be associated with telehealth use in MH consultations. A binary outcome variable was generated as telehealth (1) and face-to-face (0). Independent variables in the model included sociodemographic characteristics (age, sex, SES, region, state), encounter characteristics, year, and type of MH encounter. Month was also included to account for time-associated differences, including policy changes that affected telehealth use and social factors that affected accessibility. We included these variables in the model as fixed effects variables, and the general practice as a random effects variable. All encounters were used in this substudy.
The second model assessed variation in the likelihood of a video compared to a telephone consultation by sociodemographic characteristics. The rationale for this model was to assess for sociodemographic contributors to the differences in telehealth modality of a MH consultation. A binary outcome variable was generated as video (1) and telephone (0). Other independent variables and the model were as described for the first model. All telehealth encounters were used in this substudy.
In both statistical models, we reported results as odds ratios (adjusted; aOR), with 95% confidence intervals (95% CI). We conducted all analyses using Stata MP 15.1 (StataCorp, TX, USA). Normative categories (comparisons of most interest) were chosen as the reference groups in the model.
Bias
We excluded allied health services to address representativeness bias, as allied health professions are not uniformly represented in general practice and their services are also available to patients outside general practice settings. We used multivariate modelling as a measure to reduce confounding bias, by including covariates associated with the measured outcome. Stratification by state aimed to address bias which would have otherwise occurred due to differences in COVID-19 responses and case numbers.
Ethics and funding
Outcome Health received ethical approval from the Royal Australian College of General Practitioners National Research and Evaluation Ethics Committee (17-008) to use the POLAR GP data warehouse. The Macquarie University Human Research Ethics Committee Medical Sciences Committee granted approval for the project (Reference No. 5202067517176).
This project was funded and supported by Digital Health Cooperative Research Centre Limited (project ID: DHCRC-0118). DHCRC is funded under the Commonwealth’s Cooperative Research Centres Program.
Results
Study population
The study population comprised 874 249 MH consultations with sociodemographic profiles detailed in Table 1. The percentage of MH consultations by type (see Table 2) was highest for mental health treatment consultations (MHTC) in both states, followed by mental health treatment plans (MHTP) and reviews of mental health treatment plans (RoMHTP). Focused psychological strategies (FPS) accounted for less than 1% of all consultations in each state. MH consultations and percentages by modality are detailed in Table 2. Face-to-face consultations represented the highest percentage of MH consultation modality. Telephone made up 20.17% of consultations in NSW and 30.78% in Victoria; while video was used in 3.86% and 2.67% of consultations, respectively.
Table 1. Study population
| NSW (n = 296 practices) |
Victoria (n = 419 practices) |
||||
| Characteristics | Mental health consultations (total 306 407) |
% of state total | Mental health consultations (total 567 842) |
% of state total | |
| Sex | Female | 197 377 | 64.42 | 372 244 | 65.55 |
| Male | 109 030 | 35.58 | 195 598 | 34.45 | |
| Age (years) | 0–4 | 624 | 0.20 | 862 | 0.15 |
| 5–9 | 6 100 | 1.99 | 10 440 | 1.84 | |
| 10–14 | 11 481 | 3.75 | 22 106 | 3.89 | |
| 15–19 | 22 028 | 7.19 | 48 751 | 8.59 | |
| 20–24 | 30 714 | 10.02 | 61 233 | 10.78 | |
| 25–29 | 36 478 | 11.91 | 63 932 | 11.26 | |
| 30–34 | 36 440 | 11.89 | 60 689 | 10.69 | |
| 35–39 | 32 748 | 10.69 | 55 854 | 9.84 | |
| 40–44 | 27 253 | 8.89 | 47 480 | 8.36 | |
| 45–49 | 24 150 | 7.88 | 43 461 | 7.65 | |
| 50–54 | 20 705 | 6.76 | 41 119 | 7.24 | |
| 55–59 | 17 475 | 5.70 | 33 364 | 5.88 | |
| 60–64 | 13 807 | 4.51 | 26 925 | 4.74 | |
| 65–69 | 9 354 | 3.05 | 18 367 | 3.23 | |
| 70–74 | 7 171 | 2.34 | 13 948 | 2.46 | |
| 75–79 | 4 886 | 1.59 | 9 623 | 1.69 | |
| 80–84 | 2 783 | 0.91 | 5 268 | 0.93 | |
| 85+ | 2 210 | 0.72 | 4 420 | 0.78 | |
| Remoteness | Metropolitan | 288 265 | 94.08 | 486 578 | 85.69 |
| Regional/remote | 18 142 | 5.92 | 81 264 | 14.31 | |
| Socioeconomic status | Low | 28 488 | 9.3 | 39 456 | 6.95 |
| Low-mid | 43 791 | 14.29 | 46 436 | 8.18 | |
| Mid | 15 628 | 5.1 | 102 252 | 18.01 | |
| Mid-high | 55 516 | 18.12 | 146 866 | 25.86 | |
| High | 162 984 | 53.19 | 232 832 | 41.00 |
Table 2. MH consultations by service type and modality
| NSW n (%) |
Victoria n (%) |
|
| Service type | ||
| MHTC | 138 178 (45.10) | 259 896 (45.77) |
| MHTP | 116 024 (37.87) | 201 004 (35.40) |
| RoMHTP | 50 903 (16.61) | 101 601 (17.89) |
| FPS | 1302 (0.42) | 5 341 (0.94) |
| Consultation modality | ||
| Face-to-face | 232 750 (75.96) | 377 933 (66.56) |
| Telephone | 61 815 (20.17) | 174 769 (30.78) |
| Video | 11 842 (3.86) | 15 140 (2.67) |
MHTC: mental health treatment consultation, MHTP: mental health treatment plans, RoMHTP: review of mental health treatment plans, FPS: focused psychological strategies
Proportion of telehealth consultations (objective 1)
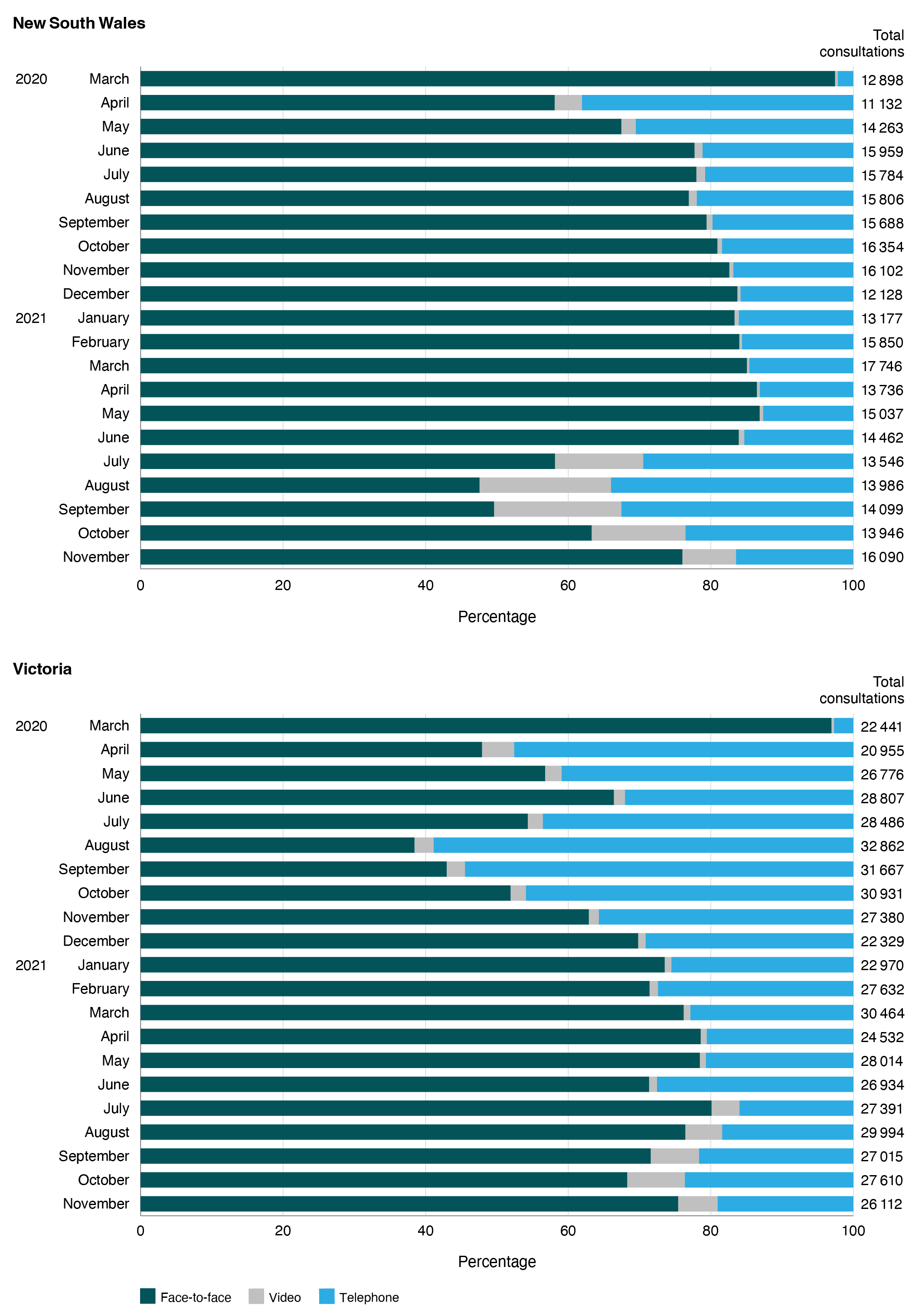
Figure 1 shows the monthly percentage of MH consultations delivered via telehealth compared with face-to-face consultations. Telehealth was adopted from the start of the pandemic with the percentage of telephone consultations higher than video across all months in both states. Telehealth use peaked in Victoria during the second wave of the pandemic restrictions, accounting for 61.6% and 57.1% of MH consultations during July and August 2020 respectively. In NSW, telehealth use peaked during August 2021, when 52.5% of MH consultations were delivered via telehealth (18.5% video, 34% telephone), coinciding with a period of stay-at-home orders during the Delta wave of the pandemic. Telehealth use continued throughout 2021 with a notable increase in video consultations from July 2021 onwards in both states, coinciding with changes to telehealth MBS item numbers that saw a reduction in the number of telephone service items (see Supplementary file Table 1B, available from: doi.org/10.25949/23826831.v1).11
Figure 1. Monthly percentage and total of mental health consultations provided by modality (face-to-face, video and telephone) in the study population between March 2020 and November 2021 in NSW and Victoria (click figure to enlarge)
Telehealth use by consultation type (objective 2)
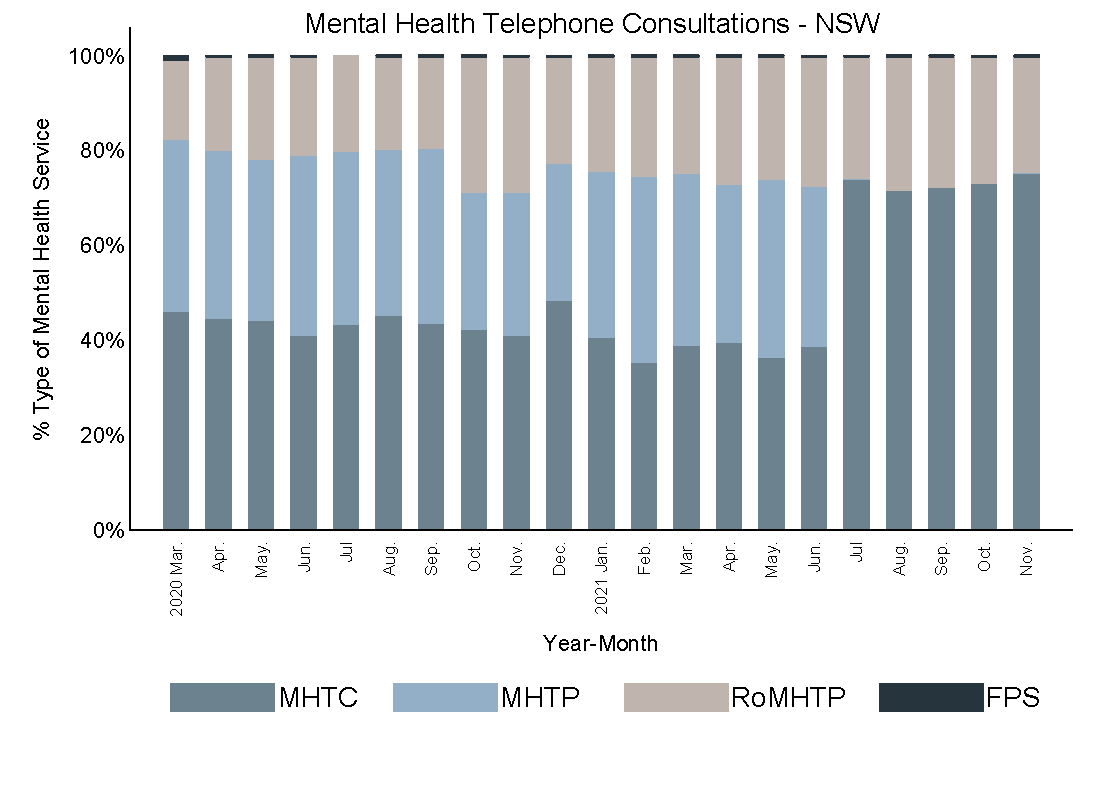
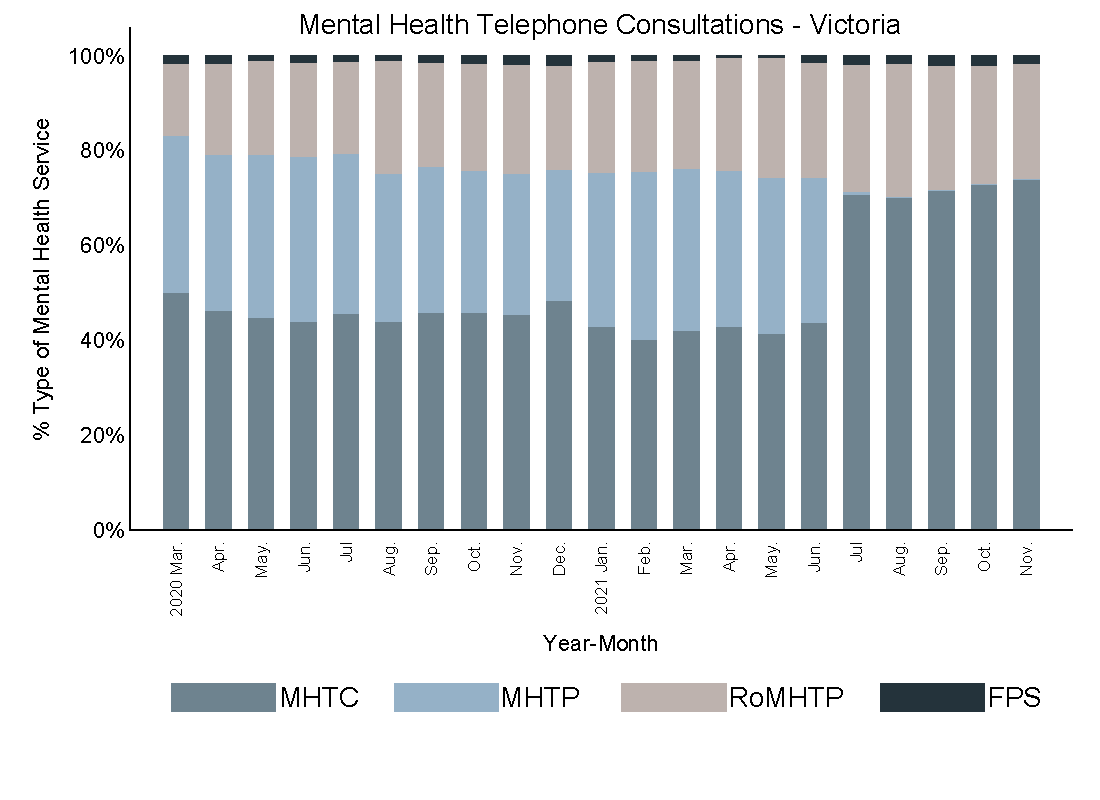
Figure 2 shows telehealth utilisation by consultation type for telephone (Panel A) and video (Panel B). Telephone was predominantly used for MHTC, followed by MHTP and RoMHTP in both states. Telephone utilisation was relatively consistent across the study period for all consultation types until the noticeable drop in the proportion of telephone MHTP consultations from July 2021 onwards. Video consultations show greater variability by consultation type across the study period with video mostly used for MHTC and MHTP in both states. There is a notable increase in the proportion of video MHTP from July 2021 onwards.
Figure 2. Monthly proportion of telephone (Panel A) and video (Panel B) consultations by mental health consultation type in NSW and Victoria between March 2020 and November 2021
Panel A: Monthly proportion of telephone consultations, NSW and Victoria (click each figure to enlarge)
Panel B: Monthly proportion of video consultations, NSW and Victoria (click each figure to enlarge)
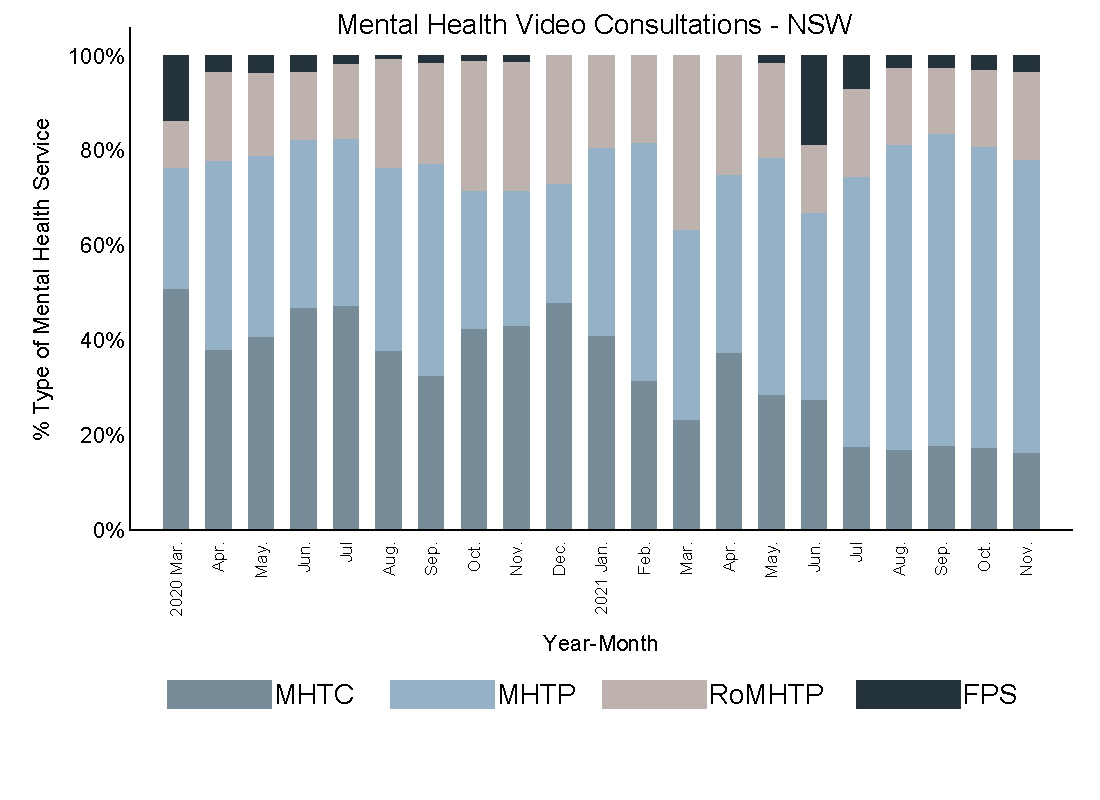
MHTC: mental health treatment consultation, MHTP: mental health treatment plans, RoMHTP: review of mental health treatment plans, FPS: focused psychological strategies
Mental health telehealth consultation demographics (objective 3)
For full results for sociodemographic variables associated with telehealth use for MH-related consultations with reference to face-to-face consultations, see Supplementary File 3, Panel A (available from: /doi.org/10.25949/23826870.v1).). Compared with females, males were less likely to use telehealth than a face-to-face consultation (aOR 0.80 95%CI: 0.79, 0.81). Compared with adults aged 25–29, youngest age groups (ages 0–4 aOR 1.70 95%CI: 1.50, 1.91; ages 5–9 aOR 1.49 95%CI: 1.43, 1.55) and ages 30–34, 35–39 and 40–44 (aORs 1.09 95%CI: 1.07, 1.12; 1.10 95%CI: 1.07, 1.12; and 1.08 95%CI: 1.06, 1.10 respectively) were more likely to use telehealth. Older adults were increasingly less likely to use telehealth with increased age (ages 50–54 aOR 0.93 95%CI: 0.91, 0.95; ages 85+ aOR 0.59 95%CI: 0.55, 0.63).
Compared with people classified as mid-SES, high-SES had a statistically significantly lower likelihood of a telehealth consultation (aOR 0.96 95%CI: 0.93, 0.98) while other SES groups had higher likelihoods (low-SES aOR 1.05 95%CI: 1.02, 1.08; low/mid-SES aOR 1.03 95%CI: 1.001, 1.06); high/mid-SES aOR 1.04 95%CI: 1.02, 1.06). Compared with metropolitan areas, regional/remote areas were more likely to have a telehealth consultation (aOR 1.25 95%CI: 1.21, 1.29). Compared with Victoria, NSW residents were less likely to have a telehealth consultation (aOR 0.82 95%CI: 0.73, 0.93). Compared with 2020, patients were less likely to use telehealth in 2021 (aOR 0.58 95%CI: 0.58, 0.59). Compared with MHTC, patients were more likely to use telehealth for FPS (aOR 1.85 95%CI: 1.74, 1.96) and RoMHTP (aOR 1.38 95%CI: 1.36, 1.40) and were less likely for use it for MHTP (aOR 0.70 95%CI: 0.70, 0.71).
For full results for sociodemographic variables associated with video consultations with reference to telephone consultations, see Supplementary File 3, Panel B available from: doi.org/10.25949/23826870.v1).
Compared with telephone, we observed no differences in the use of video for MH-telehealth consultations for sex and region. Compared with ages 25–29, ages 15–24 were more likely to use video consults (ages 15–19 aOR 1.09 95%CI: 1.02, 1.17; ages 20–24 aOR 1.16 95%CI: 1.10, 1.24) while ages 50–54 (aOR 0.86 95%CI: 0.80, 0.93) and 60+ were less likely to use video (from aOR 0.91 95%CI: 0.83, 0.99 for ages 60–64 to aOR 0.52 95%CI: 0.38, 0.71 for ages 85+).Video was more likely to be used in NSW than Victoria (aOR 1.80 95%CI: 1.47, 2.23) and was more likely to be used in 2021 than 2020 (aOR 4.82 95%CI: 4.66, 4.98). Compared with MHTC, video was more likely than telephone to be used for MHTP (aOR 5.34 95%CI: 5.14, 5.54), FPS (aOR 12.98 95% CI: 11.20, 15.03), and RoMHTP (aOR 1.39 95%CI: 1.33, 1.45).
Discussion
This retrospective observational study of 874 249 MH consultations between March 2020 and November 2021 provides a detailed understanding of telehealth utilisation for MH consultations in Australian general practice across Victoria and NSW. MH-telehealth consultations exceeded face-to-face consultations in July 2020 in Victoria during the second wave of COVID-19 and during August 2021 in NSW during the Delta wave. These findings support the important role of telehealth in enabling patient access to GPs for MH consultations during the pandemic, particularly during periods of heightened restrictions/lockdowns. MH-telehealth utilisation continued over time with telehealth providing a minimum of 13.2% and a maximum of 52.5% of monthly MH consultations in NSW, and 19.9% to 61.6% in Victoria, between April 2020 and November 2021. A sustained use of telehealth for MH consultations during 2021 has also been reported in the literature for non-GP MH providers20, and our results provide further evidence to suggest an ongoing role for telehealth in the future provision of MH services in general practice. In line with AIHW service item reports for all MH providers7, our results (Figure 1) show differences in the month-to-month percentages of telehealth use between NSW and Victoria. In Victoria, the percentage of consultations provided by telehealth shows greater temporal variation compared to NSW, where the percentage of telehealth consultations remained relatively consistent between June 2020 and June 2021. A higher percentage of video use in NSW compared with Victoria is evident between July and September 2021. These findings highlight the importance of considering the impact of contextual circumstances, such as state-level pandemic response measures/lockdowns7, the COVID-19 vaccination program17, case numbers, or changes to MBS item numbers on the use of telehealth services.
Our study results demonstrate that telephone was the predominant MH-telehealth modality in our general practice study population, which is consistent with literature for all general practice telehealth consultations.21-23 Telephone was used to provide all MH consultation types until July 2021, after which our analyses reveal a large decrease in telephone consultations and a concomitant increase in video for MHTP. These changes coincided with, and demonstrate the impact of, a national policy change to MBS telehealth items that included the cessation of selected MHTP telephone items (Supplementary File 1, available from: doi.org/10.25949/23826831.v1) from 1 July 2021.11 While the increase in video consultations from July 2021 may be attributed to the national changes to MBS MHTP telephone service items, the increase also coincided with the Delta wave of COVID-19 and ensuing state-specific public health measures. As the increase in video utilisation also occurred well into the second year of the pandemic, further evidence is needed to understand whether GPs/patients had greater confidence in the use of video as a modality or whether general practices had also increased their capacity to provide video consultations.
Studies outside the general practice setting have suggested that telehealth is not suited to all MH patients24,25and that usage may vary between age groups and sex.26 Our statistical models found an increased likelihood of telehealth use with ages 30–44 (compared with 25–29), being female, living in regional/remote areas, low-SES to high/mid-SES classifications, and residing in Victoria. Our findings for age, state and sex are consistent with evidence from a non-general practice MH study that included psychologists, occupational therapists and social workers, which reported greater telehealth (telephone and video) utilisation by females aged 25–34 and variations between Australian states/territories.26 Our results show a decrease in telehealth utilisation with increasing age from age 50 upward, which may reflect the age differences in digital ability, access and digital inclusion, as reported in the 2021 Australian digital inclusion index data dashboards.27 Additional factors that may impact telehealth use by older persons as discussed by Dykgraaf et al28, include cognitive and physical challenges, which may impact both phone and video use. Our study grouped consultations by 5-year age groups but did not differentiate between items for general MH versus specialised items (e.g. MBS items for treating eating disorders), which could be explored in future research. More granular evidence is required to understand MH-telehealth use by SES to inform whether the negative association between MH-telehealth use and high-SES (compared to mid-SES) is a feature of our study population or MH consultations in general practice.
Even though females in our study were more likely to use MH-telehealth, we found no evidence for sex differences between use of video and telephone consults. Our service data shows that telephone was the predominant MH-telehealth modality and that video, when utilised, was used most for MHTC and MHTP, possibly due to the higher number of consultations provided for these services compared with others or the changes to telephone item numbers during 2021. The likelihood of a MH-telehealth service being provided via video (compared with telephone) was highest for FPS, followed by MHTP, RoMHTP, and MHTC respectively. These findings suggest that consultation type may be an important factor in the choice of modality for MH-telehealth consultations. Although data used in this study cannot provide reasons underlying these findings, existing literature has examined patient31,32, provider24,30,31, treatment/consultation type29, social29,30, and technology/practice30,31factors associated with telehealth use. These factors all have the potential to impact choice of consultation modality.
Our findings echo the need for more MH research that directly compares telephone and video, as highlighted in the literature.29 As our study presents the sociodemographic characteristics of general practice patients who used MH-telehealth services, further research is needed to understand how individual GP/practice characteristics may have influenced MH consultation modality. Current evidence suggests practice size and GP characteristics may be related to video utilisation in general practice.31 Qualitative research could also complement our findings by exploring how MH consultation type, MH condition, reason for consultation or external factors (such as the concurrent use of non-general practice MH services), influence patients’ telehealth modality preferences, including specific patient preferences for, or practical experiences with, MH-telehealth modalities.
Strengths and limitations
The large sample size of 874 249 consultations and duration of the study time frame including analysis of data over 21 months of the pandemic are major strengths of this study. The data reflect MH consultations billed in general practice, which are indicative of patients who sought professional advice from a GP for their MH concerns and also reflect MH conditions that have been clinically diagnosed. The retrospective nature and source of the observational data overcomes selection bias that may potentially occur with survey-based data.
Limitations of the study include the possibility of an underestimation of the true number of MH consultations due to reliance on MBS billing data. This was highlighted by many of the findings of a 2021 survey report of GPs with MH skills training32 including, for example, instances where a patient may have presented with multiple health concerns and their MH concerns may have been addressed within the context of a routine consultation.32 The data do not reflect instances when a consultation started as video and then changed to telephone due to technical difficulties. Data only reflect general practice activity in participating practices, which were predominantly in metropolitan regions. Although a large number of practices are included in this study, our results may not be generalisable to other practices and states/territories. Data were subject to individual GPs’ application of the MBS billing rules34 and the severity/nature of MH conditions is unknown. When interpreting results for video consultations in March 2020, it should be noted that video only accounted for 0.4% of consultations in each state during this first month and thus the results likely reflect video use in a small number of practices.
Conclusion
The analysis of MH-telehealth consultation service data and modelling in this study portray a comprehensive picture of the temporal changes to, and sociodemographic characteristics of, MH-telehealth services in Australian general practice across the first 21 months of the COVID-19 pandemic. Although MH consultations were predominantly face-to-face during the study period, telehealth played an important role in providing access to MH services during periods of lockdown. MH-telehealth consultations exceeded face-to-face during periods of greater government public health restrictions. The continued use of MH-telehealth during periods of reduced restrictions suggests telehealth has an ongoing role in MH consultations in general practice into the future. Through understanding how telehealth has been used for MH consultations in general practice, including the characteristics of patients using telehealth modalities and the types of consultations delivered by telehealth, the study results can aid general practices, health planners/policy makers, digital health organisations, and primary health networks in planning for the future provision of MH services via telehealth.
Peer review and provenance
Externally peer reviewed, not commissioned.
Copyright:

© 2023 Thomas et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. World Health Organization. WHO Coronavirus (COVID-19) dashboard. Geneva; WHO; 2021 [cited 31 Aug 2022]. Available from: covid19.who.int/
- 2. Dawel A, Shou Y, Smithson M, Cherbuin N, Banfield M, Calear AL, et al. The effect of COVID-19 on mental health and wellbeing in a representative sample of Australian adults. Front Psychiatry. 2020;11:579985. CrossRef | PubMed
- 3. Newby JM, O’Moore K, Tang S, Christensen H, Faasse K. Acute mental health responses during the COVID-19 pandemic in Australia. PLoS One. 2020;15(7):e0236562. CrossRef | PubMed
- 4. Rogers SL, Cruickshank T. Change in mental health, physical health, and social relationships during highly restrictive lockdown in the COVID-19 pandemic: evidence from Australia. PeerJ. 2021;9:e11767. CrossRef | PubMed
- 5. Hammarberg K, Tran T, Kirkman M, Fisher J. Sex and age differences in clinically significant symptoms of depression and anxiety among people in Australia in the first month of COVID-19 restrictions: a national survey. BMJ Open. 2020;10(11):e042696. CrossRef | PubMed
- 6. Rossell SL, Neill E, Phillipou A, Tan EJ, Toh WL, Van Rheenen TE, et al. An overview of current mental health in the general population of Australia during the COVID-19 pandemic: Results from the COLLATE project. Psychiatry Res. 2021;296:113660. CrossRef | PubMed
- 7. Australian Institute of Health and Welfare. Mental health impact of COVID-19: Mental health service activity in Australia 2022 [cited 2023 Jul 25]. Available from: www.aihw.gov.au/getmedia/d2e9e5e2-969a-4dca-9b84-31b5fec33e46/Mental-health-impact-of-COVID-19.pdf.aspx
- 8. Sreedharan S, Mian M, Giles S. Mental health attendances in Australia during the COVID-19 pandemic: a telehealth success story? Asia Pac J Public Health. 2021;33(4):453–5. CrossRef | PubMed
- 9. Pearce C, McLeod A. COVID-19 and Australian general practice: mental health conditions during the pandemic. Outcome Health GP Insights paper No. 5.Victoria: Outcome Health; 2020 [cited 2021 Apr 13]. Available from: polargp.org.au/wp-content/uploads/2020/05/5_COVID19-Paper-5-Mental-Health.pdf
- 10. Australian Institute of Health and Welfare. Mental health. Medicare-subsidised mental health-specific services. Canberra; AIHW; 2022 [cited 2023 Feb 2]. Available from: www.aihw.gov.au/reports/mental-health-services/mental-health-services-in-australia/report-contents/medicare-subsidised-mental-health-specific-services
- 11. Australian Government Department of Health. COVID-19 temporary MBS telehealth services. Canberra: Department of Health; 2021 [cited 2021 Dec 6]. Available from: www.mbsonline.gov.au/internet/mbsonline/publishing.nsf/Content/0C514FB8C9FBBEC7CA25852E00223AFE/$File/Factsheet-COVID-19-GPsOMP-16.11.21.pdf
- 12. Pearce C, McLeod A, Gardner K, Supple J, Epstein D, Buttery J. The GP insights series no 7: primary care and SARS-CoV-2: The first 40 weeks of the pandemic year. Victoria: Outcome Health; 2020 [cited 2022 May 12]. Available from: polargp.org.au/wp-content/uploads/2020/11/COVID19-Paper-6-The-first-40-weeks.pdf
- 13. Ministers Department of Health and Aged Care.The Hon Greg Hunt MP. Permanent telehealth to strengthen universal Medicare. Canberra; Department of Health and Aged Care; 13 Dec 2021 [cited 2023 Jul 25]. Available from: www.health.gov.au/ministers/the-hon-greg-hunt-mp/media/permanent-telehealth-to-strengthen-universal-medicare
- 14. Australian Bureau of Statistics. COVID-19 mortality by wave. Canberra: ABS; 2022 [cited 2023 Jul 26]. Available from: www.abs.gov.au/articles/covid-19-mortality-wave
- 15. Kidd M, de Toca L. Editorial: the contribution of Australia’s general practitioners to the COVID-19 vaccine rollout. Aust J Gen Pract. 2021;50:871–2. CrossRef | PubMed
- 16. Outcome Health. POLAR by Outcome Health: Cloud-based clinical intelligence. [cited 23 January 2023]. Available from: polargp.org.au/
- 17. Pearce C, McLeod A, Rinehart N, Ferrigi J, Shearer M. What a comprehensive, integrated data strategy looks like: the Population Level Analysis and Reporting (POLAR) Program. Stud Health Technol Inform. 2019;264:303–7. CrossRef | PubMed
- 18. Australian Bureau of Statistics. Socio-Economic Indexes for Areas. Canberra: ABS; 2022 [cited 2023 Jan 30]. Available from: www.abs.gov.au/websitedbs/censushome.nsf/home/seifa
- 19. Australian Bureau of Statistics. Remoteness Structure: The Australian Statistical Geography Standard (ASGS) remoteness structure. Canberra: ABS; 2021 [cited 2023 Jan 30]. Available from: www.abs.gov.au/statistics/statistical-geography/remoteness-structure
- 20. Snoswell CL, Arnautovska U, Haydon HM, Siskind D, Smith AC. Increase in telemental health services on the Medicare Benefits Schedule after the start of the coronavirus pandemic: data from 2019 to 2021. Aust Health Rev. 2022;45(5):544–9. CrossRef | PubMed
- 21. Snoswell CL, Caffery LJ, Haydon HM, Thomas EE, Smith AC. Telehealth uptake in general practice as a result of the coronavirus (COVID-19) pandemic. Aust Health Rev. 2020;44(5):737–40. CrossRef | PubMed
- 22. Desborough J, Dykgraaf SH, Sturgiss E, Parkinson A, Dut G, Kidd M. What has the COVID-19 pandemic taught us about the use of virtual consultations in primary care? Aust J Gen Pract. 2022;51(3):179–83. CrossRef | PubMed
- 23. De Guzman KR, Snoswell CL, Smith AC. The impact of telehealth policy changes on general practitioner consultation activity in Australia: a time-series analysis. Aust Health Rev. 2022;45(5):605–12. CrossRef | PubMed
- 24. Farrer LM, Clough B, Bekker MJ, Calear AL, Werner-Seidler A, Newby JM, et al. Telehealth use by mental health professionals during COVID-19. Aust N Z J Psychiatry. 2023;57(2):230–40. CrossRef | PubMed
- 25. Nicholas J, Bell IH, Thompson A, Valentine L, Simsir P, Sheppard H, et al. Implementation lessons from the transition to telehealth during COVID-19: a survey of clinicians and young people from youth mental health services. Psychiatry Res. 2021;299:113848. CrossRef | PubMed
- 26. Jayawardana D, Gannon B. Use of telehealth mental health services during the COVID-19 pandemic. Aust Health Rev. 2021;45(4):442–6. CrossRef | PubMed
- 27. Thomas J, Barraket J, Parkinson S, Wilson C, Holcombe-James I, Kenned J, et al. Australian Digital Inclusion Index. Melbourne: RMIT, Swinburne University of Technology, and Telstra; 2021 [cited 2022 Aug 1]. Available from: www.digitalinclusionindex.org.au/interactive-data-dashboards/
- 28. Dykgraaf SH, Desborough J, Sturgiss E, Parkinson A, Dut GM, Kidd M. Older people, the digital divide and use of telehealth during the covid-19 pandemic. Aus J Gen Pract. 2022;51(9):721–4. CrossRef | PubMed
- 29. Chen PV, Helm A, Caloudas SG, Ecker A, Day G, Hogan J, et al. Evidence of phone vs video-conferencing for mental health treatments: a review of the literature. Curr Psychiatry Rep. 2022;24(10):529–39. CrossRef | PubMed
- 30. Greenhalgh T, Ladds E, Hughes G, Moore L, Wherton J, Shaw SE, et al. Why do GPs rarely do video consultations? qualitative study in UK general practice. Br J Gen Pract. 2022;72(718):e351–e60. CrossRef | PubMed
- 31. Scott A, Bai T, Zhang Y. Association between telehealth use and general practitioner characteristics during COVID-19: findings from a nationally representative survey of Australian doctors. BMJ Open. 2021;11(3):e046857. CrossRef | PubMed
- 32. The Navigators. Delivering mental health care in General practice: implications for practice and policy. Australia: General Practice Mental Health Standards Collaboration; 2021 [cited 2022 Feb 9]. Available from: gpmhsc.org.au/guidelinessection/index/bff47875-a424-4dd4-ba72-f7423fbdd029