Abstract
Objective and importance of the study: In Australia, preventable causes of morbidity and mortality are common among men. The National Men’s Health Strategy 2021–2030 highlights the need to successfully engage men in disease prevention; hence, we aimed to examine the prevention priorities, attitudes and information sources reported by Australian men.
Study type: Population survey.
Methods: Men aged 18 years and over were recruited from the nationally representative Life in Australia panel. Participants completed an online survey that measured the prevention issues of greatest concern, attitudes to prevention behaviours and services, and the health information sources considered most useful.
Results: Among 1282 respondents, mental health issues, followed by those pertaining to chronic disease and relationships, were rated of highest concern. Weight management, physical activity, and fruit and vegetable consumption were most often considered as important for personal health. Being 65 years and older and having adequate health literacy were strongly associated with positive attitudes towards prevention practices. More than three-quarters of men rated their doctor as the most useful information source, followed by health websites, internet searching, and their partner.
Conclusions: Psychological and social issues are of high concern to men, and their attitudes toward preventive behaviours and services often do not align with public health recommendations. Understanding the topics of greatest concern to men and their preferred sources of information can inform communication and engagement strategies to improve health-related practices among men.
Full text
Introduction
The health of Australian males is a national health priority. Undetected or ineffectively managed diseases pose a substantial public health burden, resulting in Australian males living, on average, nearly 5 years less ‘healthy life’ than females.1 Australian men are twice as likely as women to die before 75 years from preventable causes.2 Addressing the burden of preventable disease in men is a priority for the Australian Government, recognised in the National Men’s Health Strategy 2020–2030 (NMHS).3
The foremost objective of the NMHS is to empower and support men and boys to optimise their health and wellbeing across the life course. A foundational principle that it sets down to achieve this is to consider the needs and preferences of men in information provision, programs and services. There is an understanding that low attention to health information4 and delayed use of healthcare services5 have contributed to poor health outcomes among men, which must be redressed. Following best practice guidance for public communication6 and community engagement7, the NMHS acknowledges that strategies to disseminate health information and mobilise men to use preventive services should take account of their existing interests and concerns if they are to have salience and impact.
A wide body of literature identifies traditional masculine norms, including self-reliance, strength and stoicism, as factors that inhibit men’s use of health information and services.8 However, it has been argued that these hegemonic constructions of masculinity do not adequately account for the male population’s multiple forms of masculinity (and associated values and practices).9 The NMHS places strong emphasis on taking account of diversity among Australian men, but thus far, there is little population-level research about the range of preferences, attitudes and priorities that affect men’s attention to health issues, and prevention in particular. The small and/or geographically limited studies conducted in Australia indicate that men look to their general practitioner (GP) as a primary source of health information and most often identify stress as a health issue of concern. It has also been reported that men’s beliefs and preferences vary by age and the nature of the health issues.10,11
This study aimed to investigate Australian men’s health preferences and priorities to inform strategies to increase their engagement with preventive health information and services. Importantly, this examines how prevention concerns, attitudes, and information sources differ by age and by men’s social and cognitive characteristics.
Methods
Study design and ethics
A national cross-sectional survey was conducted, with approval by the Monash University Human Research Ethics Committee (No. 27289).
Participants and sampling
Study participants were males aged 18 years and over who were proficient in English and had access to telephone and internet. Men were enrolled from the Life in Australia (LiA) panel12, established in 2016 by the Social Research Centre. This comprises a probabilistic sample of more than 4000 people recruited using random digit dialling (RDD) with a 30:70 split between landline and mobile numbers. This panel has been refreshed in 2018, 2019 and 2020 using a mix of probabilistic methods (e.g., mobile RDD, Geocoded National Address database).
All men in the LiA panel (N = 1409) were invited to take part by email and text message, with telephone follow-up of nonresponders. Invitations included a link to a participant information statement, with consent confirmed when men clicked forward to complete the survey. A A$10 voucher or donation to charity was offered to incentivise participation.
Survey measures
Survey development was undertaken by Healthy Male13, a national men’s health organisation funded by the Australian Government Department of Health. This entailed consultation with its medical and allied health advisors about evidence needs relevant to the NMHS, and a scan of population-based studies of males in Australia to identify evidence gaps. Following this, a systematic search of peer-reviewed and grey literature was performed to identify potential measures for inclusion in the survey.
A newly developed measure of preventive health priorities required respondents to select three issues of most concern from a list of 20 options in the domains of chronic disease, mental health, sexual health, relationships, and injury and risk-taking, or to select ‘Other’ and nominate additional issues. Personal attitudes to preventive health practices were measured by asking respondents to rate the importance (on a 7-point scale) of 12 actions for the maintenance of personal health, which included health behaviours (e.g., weight management, limiting alcohol intake) and use of preventive care services (e.g., annual GP visits, skin checks). Preferred sources of health information were determined by asking respondents to nominate the three most useful sources from 18 choices or to select ‘Other’ and specify the source. These measures are available in Supplementary Table 1 (available from: doi.org/10.26180/24209313).
Additional measures included health literacy, using the 16-item European Health Literacy Survey Questionnaire14, and knowledge about the preventability of major causes of disease and injury.15 Demographic information collected included age, postcode of residence, marital status, educational attainment, occupation, and country of birth. Respondents were also asked whether they lived with selected disabilities and/or chronic physical and mental health conditions.
The clarity and acceptability of the survey instrument was pre-tested through online administration to an age-stratified sample of men (N = 40) and follow-up interviews with a sub-sample of respondents (N = 13). The survey was administered in March 2021.
Data analysis
Data were weighted to the profile of the Australian men (using Australian Bureau of Statistics, 2020, reference data) by age, country of birth, geographic distribution, educational attainment, socioeconomic index for areas (SEIFA), telephone access, and duration at current residence. Prevalence calculations were made for: the preventive health issues ranked as the greatest concern; preventive health behaviours and services rated as having high personal importance; and health information sources ranked as most useful. Stratified analysis was undertaken by: age group; location of residence (urban or regional/rural); marital status; SEIFA quintile; educational attainment; occupational category; country of birth (English-speaking or other); and disability and chronic condition status. For selected variables, stratification was also undertaken by health literacy (inadequate vs. adequate) and prevention knowledge (high vs. moderate/low). Bivariate differences were examined using Chi-square, and independent relationships between variables were assessed using forced entry logistic regression. Data were analysed using IBM SPSS V28.0.
Results
Study participants
Of 1409 invited males, 91% (n = 1282) completed the survey. Prior to weighting, the sample had good demographic representation (Table 1). Weighting to the Australian population resulted in higher relative proportions of respondents aged 18–34 years, never married, in the lowest two quintiles of SEIFA, who had vocational or high school level education, worked in trades/manual or sales/service occupations, and who were born in a non-English speaking (NES) country. Weighting lowered the proportion of men living with a chronic physical condition.
Table 1. Characteristics of survey participants (N = 1282)
| Demographic and health factors | Characteristics | N a | Unweighted % |
Weighted % |
| Age (years) | 18–34 | 185 | 14.5 | 30.8 |
| 35–49 | 294 | 23.0 | 25.4 | |
| 50–64 | 385 | 30.1 | 23.6 | |
| 65 and older | 414 | 32.4 | 20.2 | |
| Residential location | Urban | 874 | 68.3 | 66.6 |
| Rural | 406 | 31.7 | 33.4 | |
| Marital status | Never married | 193 | 15.1 | 22.4 |
| Married/partner | 943 | 73.9 | 67.7 | |
| Divorced/widowed | 140 | 11.0 | 9.9 | |
| SEIFA quintile | Q1 (lowest) | 197 | 15.4 | 19.1 |
| Q2 | 214 | 16.7 | 20.0 | |
| Q3 | 240 | 18.8 | 19.8 | |
| Q4 | 275 | 21.5 | 20.6 | |
| Q5 (highest) | 352 | 27.5 | 19.9 | |
| Education | University | 613 | 49.4 | 33.2 |
| Vocational | 366 | 29.5 | 38.8 | |
| High school | 262 | 21.1 | 28.1 | |
| Occupation | Manager/professional | 738 | 57.6 | 47.5 |
| Trades/manual | 321 | 25.1 | 30.5 | |
| Sales/service | 198 | 15.5 | 18.8 | |
| Other | 24 | 1.9 | 3.2 | |
| Country of birth | English speaking | 1066 | 83.4 | 77.3 |
| Non-English speaking | 212 | 16.6 | 22.7 | |
| Disabilityb | Living with a disability | 313 | 24.4 | 22.3 |
| Chronic diseasec | Physical condition | 674 | 52.6 | 45.5 |
| Mental condition | 191 | 14.9 | 16.7 |
a Factors with totals less than 1282 are due to missing data
b Total respondents reporting they are living with a disability
c Total respondents reporting they lived with a chronic disease or a mental health condition
Q=quintile; SEIFA= socioeconomic index for areas
Preventive health priorities
Stress was the most frequently identified preventive health issue, followed by exercise, depression, weight control, anxiety, diet and loneliness (Table 2). Issues related to injuries, risk-taking, and sexual health were rated as the lowest concern, identified by less than 10% of men.
Stress, anxiety and loneliness were more often rated as a high concern by men aged 18–34 years than those in the older age groups. Men aged 35–49 years had greater levels of concern about depression, parenting, and managing anger, while those aged 50–64 years more often rated weight control, alcohol intake, partner relationships and erectile dysfunction as of high concern. Men aged 65 years and older had the highest prevalence of concerns about exercise, weight control, body image and erectile dysfunction.
Multivariable analysis revealed that those aged over 50 years had the greatest concern about chronic disease issues (Supplementary Table 1 available from doi.org/10.26180/24209313). In contrast, those in the youngest age group or with a chronic mental health condition most often reported concerns about mental health. The absence of a chronic physical or mental condition was associated with greater concern about social relationships, whereas being married or living with a partner was associated with not having concerns about relationships. Vocational level education and working in a trade or manual occupation were most strongly associated with concern about injury and risk-taking, while being 65 years and over and working in a trade or manual occupation had the strongest association with concern about sexual health issues.
Personal importance of health behaviours and preventive services
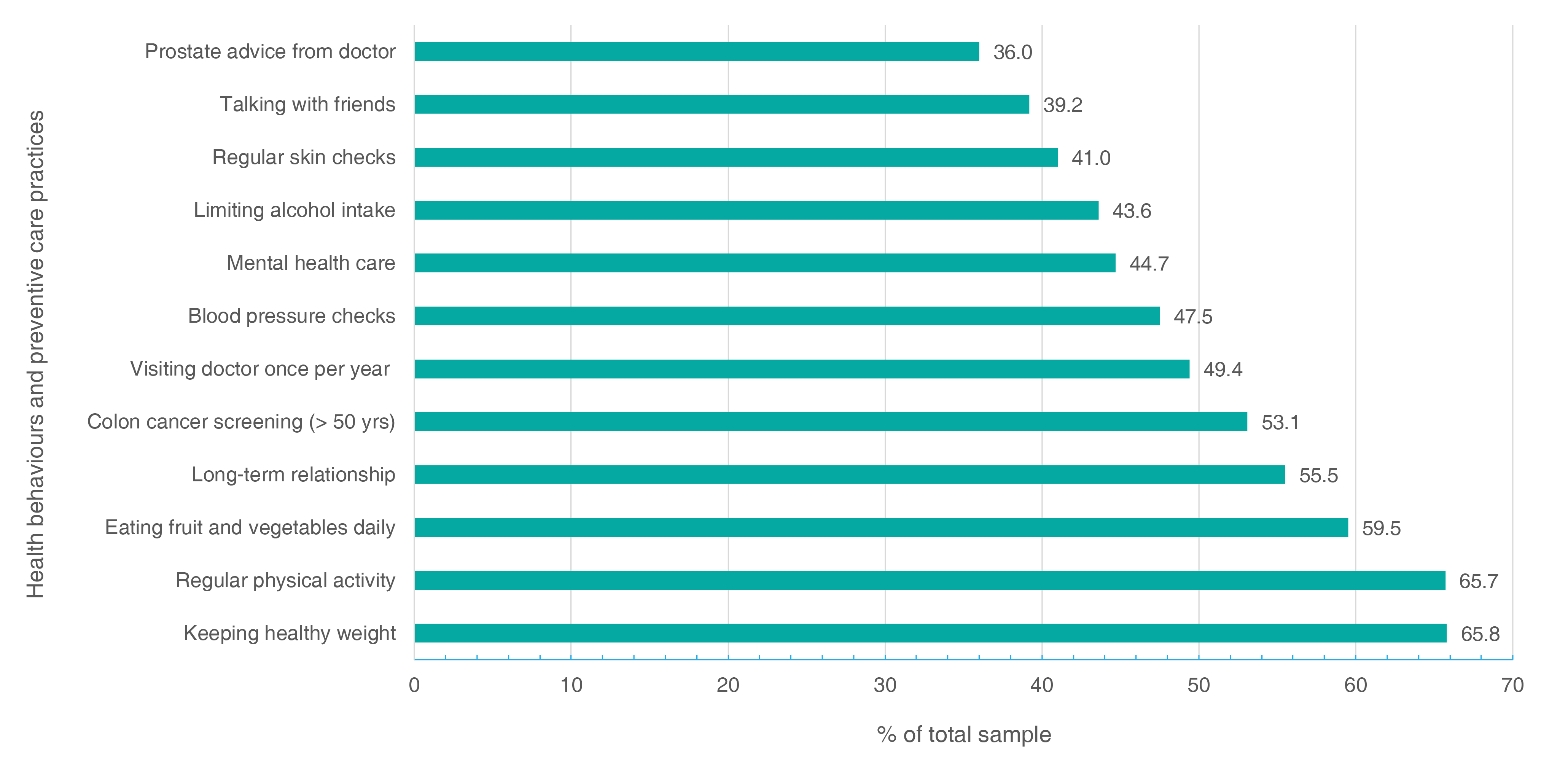
Maintaining a healthy weight and undertaking regular physical activity were the actions that men most often rated as highly important for maintaining personal health, with each nominated by about two-thirds of respondents (Figure 1). Eating fruits and vegetables and being in a long-term relationship were the next most highly rated. Limiting alcohol intake was rated as important by two in five men. Just over half of men rated colon cancer screening from age 50 as an important preventive care practice, while fewer men rated other types of health checks and screening practices (e.g., annual doctor visits, skin checks) as important.
Being aged 65 years and over, having a high level of prevention knowledge and adequate health literacy were consistently associated with placing importance on different health behaviours in multivariable analysis (Supplementary Table 2, available from: doi.org/10.26180/24209313). Being in the top quintile of SEIFA was associated with prioritising a healthy weight and regular physical activity. Men who were married or living with a partner showed a higher likelihood of rating a long-term relationship as important, while being born in an NES country and being in the lowest SEIFA quintile was associated with placing importance on limiting alcohol intake.
The youngest-aged men were least likely to rate preventive health checks and screening activities as personally important, with the likelihood increasing with age (Supplementary Table 3, available from: doi.org/10.26180/24209313). Men with adequate health literacy were more likely to rate all types of preventive service use as important. Men from NES countries were more likely to rate annual doctor visits, blood pressure checks and seeking mental health care as personally important.
Table 2. Preventive health issues rated as highest priorities by men
| Issue | All men | 18–34 years | 35–49 years | 50–64 years | 65 years+ | |||||
| %a | Rank overall | %a | Rank /10 | %a | Rank /10 | %a | Rank /10 | %a | Rank /10 | |
| Mental health | ||||||||||
| Stress | 40.8 | 1 | 52.2 | 1 | 42.9 | 1 | 36.4 | 2 | 25.2 | 3 |
| Depression | 31.9 | 3 | 34.5 | 2 | 38.2 | 2 | 34.6 | 4 | 16.3 | 8 |
| Anxiety | 26.7 | 5 | 33.3 | 3 | 27.3 | 5 | 20.0 | Equal 5/6 | 23.0 | 5 |
| Body image | 12.4 | 9 | 13.6 | 8 | – | – | – | – | 18.8 | 6 |
| Chronic disease | ||||||||||
| Exercise | 33.5 | 2 | 29.9 | 4 | 28.4 | 4 | 37.5 | 1 | 41.1 | 1 |
| Weight control | 30.3 | 4 | 21.1 | 6 | 30.1 | 3 | 35.4 | 3 | 38.8 | 2 |
| Diet | 18.0 | 6 | 19.6 | 7 | 20.6 | 6 | 16.5 | 7 | 14.0 | 9 |
| Alcohol intake | 14.5 | 8 | 10.5 | 9 | 11.1 | 10 | 20.0 | Equal 5/6 | 18.3 | 7 |
| Smoking | 6.9 | Equal 14/15 | – | – | – | – | 10.0 | 10 | – | – |
| Relationships | ||||||||||
| Loneliness | 15.3 | 7 | 22.1 | 5 | 15.1 | 7 | – | – | 12.9 | 10 |
| Partner relations | 10.8 | 10 | 10.6 | 10 | – | – | 14.5 | 8 | – | – |
| Parenting | 6.9 | Equal 14/15 | – | – | 13.7 | 8 | – | – | – | – |
| Injuries/risk-taking | ||||||||||
| Managing anger | 8.7 | 12 | – | – | 11.5 | 9 | – | – | – | – |
| Work safety | 8.1 | 13 | – | – | – | – | – | – | – | – |
| Recreational drugs | 3.4 | 16 | – | – | – | – | – | – | – | – |
| Performance drugs | 0.4 | 20 | – | – | – | – | – | – | – | – |
| Sexual health | ||||||||||
| Erectile dysfunction | 8.8 | 11 | – | – | – | – | 12.3 | 9 | 24.4 | 4 |
| Premature ejaculation | 4.0 | 17 | – | – | – | – | – | – | – | – |
| Fertility | 1.6 | 18 | – | – | – | – | – | – | – | – |
| Sexually transmitted infections | 1.4 | 19 | – | – | – | – | – | – | – | – |
– Blank cells indicate that source not ranked as one of top 10 most useful.
a Percentage who rated the source in their top three information sources.
Figure 1. Health behaviours and preventive care practices rated as very important for personal health (N = 1282) (click figure to enlarge)
Preferred sources of information
More than three-quarters of men nominated advice from their doctor as the most useful source of information, followed by the websites of health agencies, web browsing, their partners and family members (Table 3). Overall, information sources in the clinical or health service category were most often ranked as highly useful, and social media information sources the least often.
The proportion of men who ranked doctor advice and their partner as very useful increased with age. Men in the youngest age group often nominated web browsing and video channels as useful information sources.
In multivariable analysis, it was found that being aged 50 years and older, as well as having a mental health condition, an English speaking-background or vocational-level education, were related to ranking a clinical information source as very useful (Supplementary Table 4, available from: doi.org/10.26180/24209313). Those aged 50–64 years were most likely to rank a health agency source as very useful, while being aged 18–34 years or born in an NES country was strongly associated with a preference for online and mass media sources. Being married or living with a partner was strongly related to ranking lay sources of information (e.g., partner, family) as very useful. Several factors were associated with ranking social media sources highly, including: age of 18–34 years; NES country of origin; and working in a sales/service occupation.
Table 3. Sources of health information identified as most useful by men
| Information sources | All men | 18–34 years | 35–49 years | 50–64 years | 65 years+ | |||||
| %a | Rank overall | %a | Rank /10 | %a | Rank/10 | %a | Rank /10 | %a | Rank /10 | |
| Clinical | ||||||||||
| Doctor advice | 78.0 | 1 | 65.8 | 1 | 73.2 | 1 | 86.1 | 1 | 93.9 | 1 |
| Health agencies | ||||||||||
| Health websites | 42.0 | 2 | 40.3 | 3 | 42.4 | 3 | 48.6 | 2 | 37.0 | 3 |
| Fact sheets | 17.7 | 6 | 13.0 | 8 | 14.8 | 8 | 22.9 | 5 | – | – |
| Brochures | 8.8 | 9 | – | – | – | – | 11.1 | 8 | – | – |
| Seminars | 5.9 | 10 | – | – | 8.8 | 9 | – | – | 4.7 | 10 |
| Helplines | 3.2 | 14 | – | – | – | – | – | – | – | – |
| Digital and mass media | ||||||||||
| Web browsing | 41.6 | 3 | 49.3 | 2 | 43.4 | 2 | 39.1 | 3 | 29.0 | 4 |
| Video channels | 10.8 | 8 | 16.3 | 6 | 15.8 | 6 | 5.9 | 9 | – | – |
| Podcasts | 4.6 | 12 | – | – | – | – | – | – | – | – |
| Mobile apps | 3.5 | 13 | – | – | – | – | – | – | – | – |
| Magazines | 2.0 | 16 | – | – | – | – | – | – | 5.1 | 9 |
| Lay sources | ||||||||||
| Partner | 30.9 | 4 | 27.3 | 4 | 28.4 | 4 | 30.4 | 4 | 39.4 | 2 |
| Family members | 22.7 | 5 | 23.4 | 5 | 23.8 | 5 | 18.9 | 6 | 24.3 | 5 |
| Friends/colleagues | 14.8 | 7 | 13.3 | 7 | 15.1 | 7 | 14.6 | 7 | 17.0 | 7 |
| Social media | ||||||||||
| 5.5 | 11 | 7.7 | 9 | 7.6 | 10 | 4.6 | 10 | – | – | |
| 2.6 | 15 | 7.6 | 10 | – | – | – | – | – | – | |
| 1.3 | 17 | – | – | – | – | – | – | – | – | |
| Twitter/X | 0.2 | 18 | – | – | – | – | – | – | – | – |
– Blank cells indicate that source not ranked as one of top 10 most useful.
a Percentage who rated the source in their top three information sources.
Discussion
Effective public communication and community engagement strategies will be required to meet the objectives of the NMHS, and these efforts should be based on an understanding of the existing health priorities and attitudes of men across diverse ages and backgrounds. This is, we believe, the first population study in Australia to elicit these insights, which can inform strategies to tackle the high burden of preventable disease and injury among men.
Three of the top five public health issues of concern to men were aspects of mental health. Stress was the most frequently nominated issue, consistent with the findings of an earlier survey of Australian men in Newcastle, NSW.10 Notably, the priority placed on mental health issues was highest among young men (18–34 years), which accords with evidence that young people most frequently report psychological distress and mental disorders.16 Given the stigma attached to loneliness, which likely contributes to an underreporting of this problem among men17, it was unexpected that this would be frequently nominated as an issue of concern. These findings clearly imply that psychological and social issues should be given prominence in health promotion strategies, for younger men in particular, to improve their relevance and population engagement.
Unsurprisingly, behaviours related to the prevention of chronic conditions were of greatest concern to older men. The ranking of erectile dysfunction as the fourth most important issue for men 65 years and over confirms previous findings.18 This highlights an opportunity for engagement with older men, not only to promote sexual health but to increase recognition of erectile dysfunction as a marker of chronic disease development.19
The frequent rating of weight management, physical activity and fruit and vegetable consumption as important for personal health may reflect extensive media coverage of these issues.20,21 However, more than one-third of men did not rate these behaviours as important, and more than half did not prioritise limiting their alcohol intake. Alcohol consumption serves multiple purposes, including stress relief and social connection, which may lead men to downplay public health recommendations about alcohol intake.22
Another concerning finding was that more than half of men did not rate using a number of preventive health services as personally important. A recent review reported that men commonly view primary health care services as a source of acute care rather than preventive checks and advice.23 This highlights the importance of applying research insights into how primary care services can be delivered in gender-appropriate ways for males 24 and exploring new models for male-friendly health services.25 In addition, there is the need for targeted communication and community engagement strategies for younger men, who were least likely to have positive attitudes towards preventive care. Notably, health literacy showed a consistently positive relationship with attitudes to prevention practices, which indicates that population-level health literacy strategies, as called for in Australia’s National Preventive Health Strategy 2021–3026, are warranted.
Although only half of men had positive attitudes to annual general practice attendance, doctors were most often identified as their preferred source of health information, consistent with previous research.10 The implications of this are twofold: the requirement to build the capacity of primary health care services to provide preventive health advice and support; and promoting timely and consistent use of these services by men. Online sources of health information were often rated as very useful, with web browsing and online video channels ranked most highly by those aged 18–34 and 35–49 years. The high rating of the usefulness of the websites of health agencies was unexpected but consistent with past findings that credibility influences online health information seeking.27 Lay sources, particularly partners, were also ranked among the most useful sources of health information. This suggests that seeking to engage partners within health promotion programs for men may strengthen their reach and impact, which warrants attention in developing and evaluating future strategies.
A strength of this study is that probabilistic sampling was used, and with population weighting, the sample generally matched the characteristics of Australian men. However, the survey was conducted in English only; consequently, men with low English proficiency were not included. Several survey measures were newly developed or adapted from existing measures. While these underwent face and content validity assessment, their reliability or validity has not been tested psychometrically.
Conclusion
Empowering men and boys to optimise their health across the life course is a foremost objective of the NMHS. The Strategy recognises that this requires attention to the needs and priorities of men and an understanding of their diversity across the population. This study reveals the issues that subgroups of men are most ready to respond to, and these insights can be applied in the development and formative testing of public communication and community engagement strategies to promote the uptake of preventive care practices by men. Online and lay sources of awareness raising (especially partners) should be used in these efforts to reach younger men alongside established health and medical information channels. This research provides timely evidence to guide the design and implementation of critical population health improvement strategies for Australian men.
Acknowledgements
Healthy Male, the organisation that conducted this national survey, is funded by the Australian Government Department of Health. Contributions from medical, nursing and allied health advisors of Healthy Male towards the development of the survey are acknowledged.
BS is an Editorial Board member and Associate Editor with PHRP. He was not involved in review and decisions on this manuscript.
Peer review and provenance
Externally peer reviewed, not commissioned.
Copyright:

© 2023 Smith et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Australian Institute of Health and Welfare. The health of Australia’s males: 25 years and over. Canberra: AIHW; 2013 [cited 2023 Sep 18]. Available from: www.aihw.gov.au/reports/men-women/the-health-of-australia-s-males-25-years-and-over/contents/table-of-contents
- 2. Pirkis J, MacDonald J, English DR. Introducing Ten to Men, the Australian longitudinal study on male health. BMC Public Health. 2016;16:1044. CrossRef | PubMed
- 3. Australian Government Department of Health. National men's health strategy 2020–2030; 2019[cited 2022 Oct 31]. Available from: www.health.gov.au/sites/default/files/documents/2021/05/national-men-s-health-strategy-2020-2030_0.pdf
- 4. Manierre MJ. Gaps in knowledge: tracking and explaining gender differences in health information seeking. Soc Sci Med. 2015;128:151–8. CrossRef | PubMed
- 5. Yousaf O, Grunfeld EA, Hunter MS. A systematic review of the factors associated with delays in medical and psychological help-seeking among men. Health Psychol Rev 2015;9(2):264–76. CrossRef | PubMed
- 6. World Health Organisation. WHO strategic communications framework for effective communications. 2017 [cited 2023 Sep 18]. Available at: cdn.who.int/media/docs/default-source/documents/communication-framework.pdf?sfvrsn=93aa6138_0
- 7. National Institute for Health and Care Excellence. Community engagement: improving health and wellbeing and reducing health inequalities. NICE guideline, 4th March 2016 [cited 2023 Sep 18]. Available from: www.nice.org.uk/guidance/ng44
- 8. Courtenay WH. Constructions of masculinity and their influence on men's well-being: a theory of gender and health. Soc Sci Med. 2000;50:1385–401. CrossRef | PubMed
- 9. Smith JA. Beyond masculine stereotypes: moving men's health promotion forward in Australia. Health Promot J Austr. 2007;18:20–5. CrossRef | PubMed
- 10. Fletcher RJ, Higginbotham N, Dobson A. Men’s perceived health needs. J Health Psychol. 2002;7(3):233–41. CrossRef | PubMed
- 11. Hodyl NA, Hogg K, Renton D, von Saldern S, McLachlan R. Understanding the preferences of Australian men for accessing health information. Aust J Prim Health. 2020;26(2):153–60. CrossRef | PubMed
- 12. Social Research Centre, Australian National University: Life in Australia panel Canberra: ANU; 2012–2023. [cited 2023 Sept 13]. Available from: srcentre.com.au/our-research/life-in-australia-panel
- 13. Healthy Male: generations of healthy Australian men. Canberra: Healthy male; 2023 [cited 2023 Sept 13]. Available from: www.healthymale.org.au
- 14. Pelikan JM, Ganahl K. Measuring health literacy in general populations: primary findings from the HLS-EU Consortium’s health literacy assessment effort. Stud Health Technol Inform. 2017;240:34–59. CrossRef | PubMed
- 15. Smith B, Sullivan E, Bauman A, Powell-Davies G, Mitchell J. Lay beliefs about the preventability of major health conditions. Health Educ Res. 1999;14(3):315–25. CrossRef | PubMed
- 16. Australian Bureau of Statistics. National study of mental health and wellbeing: summary statistics on key mental health issues including the prevalence of mental disorders and the use of services; reference period 2020–21.Canberra: ABS; 2022 [cited 2022 Oct 31]. Available from:www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/latest-release
- 17. Nicolaisen M, Thorsen K. Who are lonely? Loneliness in different age groups (18–81 years old), using two measures of loneliness. Int J Aging Hum Dev. 2014;78:229–57. CrossRef | PubMed
- 18. Holden CA, Allan CA, McLachlan RI. Windows of opportunity: a holistic approach to men's health. Med J Aust. 2010;192(12):708–11. CrossRef | PubMed
- 19. Chew KK, Finn J, Stuckey B, Gibson N, Sanfilippo F, Bremner A, et al. Erectile dysfunction as a predictor for subsequent atherosclerotic cardiovascular events: findings from a linked-data study. J Sex Med. 2010;7(1):192–202. CrossRef | PubMed
- 20. Bonfiglioli CM, Smith BJ, King LA, Chapman SF, Holding SJ. Choice and voice: obesity debates in television news. Med J Aust. 2007;187(8):442–5. CrossRef | PubMed
- 21. O’Hara BJ, Grunseit A, Phongsavan P, Bellew W, Briggs M, Bauman AE. Impact of the Swap It, Don’t Stop It Australian national mass media campaign on promoting small changes to lifestyle behaviors. J Health Commun. 2016;21(12):1276–85. CrossRef | PubMed
- 22. Parke H, Michalska M, Russell A, Moss AC, Holdsworth C, Ling J, et al. Understanding drinking among midlife men in the United Kingdom: a systematic review of qualitative studies. Addict Behav Rep. 2018;8:85–94. CrossRef | PubMed
- 23. Mursa R, Patterson C, Halcomb E. Men's help‐seeking and engagement with general practice: an integrative review. J Adv Nurs. 2022;78:1938–53. CrossRef | PubMed
- 24. Smith JA, Braunack‐Mayer AJ, Wittert GA, Warin MJ. Qualities men value when communicating with general practitioners: implications for primary care settings. Med J Aust. 2008;189:618–21. CrossRef | PubMed
- 25. Vincent AD, Drioli-Phillips PG, Le J, Cusack L, Schultz TJ, McGee MA, et al. Health behaviours of Australian men and the likelihood of attending a dedicated men’s health service. BMC Public Health. 2018;18:1078. CrossRef | PubMed
- 26. Australian Government Department of Health. National Preventive Health Strategy 2021–2030. Canberra; Department of Health; 2021 [cited 2022 Oct 31]. Available from: www.health.gov.au/sites/default/files/documents/2021/12/national-preventive-health-strategy-2021-2030_1.pdf
- 27. Sbaffi L, Rowley J. Trust and credibility in web-based health information: a review and agenda for future research. J Med Internet Res. 2017;19(6):e7579. CrossRef | PubMed