Abstract
Objectives: To provide an overview of the current state of funding for health policy and systems research (HPSR) on a national level across the Eastern Mediterranean region (EMR), and to examine the key factors influencing funding for HPSR in the region.
Methods: A multistep approach was employed, involving a documentation review, secondary data analysis and key informant interviews with 35 stakeholders from five countries in the EMR. Findings are presented narratively (and where applicable as percentages).
Results: National funding for research and development (R&D) in general, and for health research in particular, has been low in comparative terms and lagging behind at the global scale, while funding for HPSR has been lacking on a national level. None of the 22 EMR countries studied had explicit national funding or a budget line for HPSR. Analysis of funding sources of 1821 published HPSR articles in the EMR (2010–2019) showed that the most notable source was external/international grants (45.6%), followed by university/academia (35.1%), and government (9.5%). Although HPSR publications have been increasing over time, this still falls short of the scale needed for strengthening health systems and informing current transformations in the region. Findings from the interviews identified several factors influencing investment in or funding for HPSR in the EMR.
Conclusions: Many of the EMR’s policy priorities are related to health systems, however our research finds that overall investment in health research and HPSR is still low, with limited recognition of the importance of HPSR in the EMR.
Full text
Introduction
Health policy and systems research (HPSR) has the potential to provide evidence to improve decision making, strengthen health systems and improve population health outcomes.1,2 HPSR is defined as the production and application of knowledge to improve how societies organise themselves to achieve collective health goals. It is interdisciplinary and encompasses research on the policies, organisations, programs and actors that make up health systems, and examines how the interactions among these elements – and the broader determinants of health – influence health system performance.1,3
The advancement of HPSR is greatly dependent on the availability of adequate and reliable funding.4 Despite calls for increased investment in HPSR, little work has been done to date on HPSR funding in the Eastern Mediterranean region (EMR). Of the many challenges facing HPSR in the EMR, funding limitations remain the main issue.5
The overall aim of this study is to gain a better understanding of the current state of HPSR funding on a national level across the EMR. The EMR is taken to include all countries established within the World Health Organization (WHO) Regional Office for the Eastern Mediterranean (EMRO): Afghanistan, Bahrain, Djibouti, Egypt, the Islamic Republic of Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Pakistan, Palestine, Qatar, Saudi Arabia, Somalia, Sudan, Syrian Arab Republic, Tunisia, the United Arab Emirates (UAE) and Yemen. The specific objectives are to: 1) provide an overview of the amount and source of funding for health research and HPSR in the EMR; 2) assess HPSR production in the EMR; 3) examine existing governance systems for health research (and HPSR); and 4) explore key factors influencing investment in or funding of HPSR in the region.
Methods
We employed a multistep approach involving documentation review, secondary data analysis and key informant interviews. Triangulation among the multiple sources of data helped minimise bias, provide indepth data and increase the reliability, validity and consistency of findings through cross-checking of information across different data sources.
Data collection
We used PubMed, Web of Science, the Index Medicus for the EMR (IMEMR) and Google Scholar to search for published literature on HPSR in the region. The electronic database search combined both index terms and free-text words relating to the following: 1) EMR countries and 2) HPSR; which retrieved 1821 published articles on HPSR in the EMR. In addition, governmental and ministerial websites and national science funding agency websites within each country were searched for relevant reports on funding (amount, source, allocation criteria) and governance-related information for health research and HPSR (see Supplementary file 1, available from: hdl.handle.net/10938/23237). Specific searches were also conducted for relevant documents produced by the WHO (including WHO EMRO), UN agencies, and World Bank on research funding in the EMR, including HPSR. Because of the anticipated limited published data relating to HPSR funding, we expanded the search to encompass health research funding and research funding in general within each EMR country. The search was restricted to studies in the past decade (2010–2019) in the EMR.
Key informant interviews were conducted with 35 selected stakeholders from Egypt (n = 8), Iran (n = 10), Lebanon (n = 5), Palestine (n = 7) and Sudan (n = 5). This selection was a representative number of countries from the WHO EMRO region following the original study design. We could not engage stakeholders from high-income countries because of a delay of response. The stakeholders represented the following categories, which served as a sampling framework for selective invitation of participants from each country: health policy makers (n = 5); national health institutes/research centres (n = 16), researchers (n = 8) and public health professionals (n = 6).
The interviews were conducted by the local focal point and were guided by a standard interview guide (see Supplementary file 2, available from: hdl.handle.net/10938/23237). The interviews served to validate findings emerging from documentation review as well as gain insights on key factors influencing investment in or funding of HPSR in the region. The interviews were conducted virtually (via the Zoom video platform [San Jose, CA: Zoom Video Communications Inc]) and were 40–60 minutes in duration.
Data analysis
Data from the documentation review were extracted on the following variables (with the most recently available data used for each country):
- Amount of funding: Research and development (R&D) expenditure as percentage of Gross Domestic Product (GDP); absolute values of funding for research; health research and HPSR; health research expenditure as percentage of total research expenditure and health research expenditure as a percentage of country GDP
- Source of funding for published HPSR studies (from the electronic database search)
- Governance-related information: national research plan/strategy; national health research institute/council; health research promotion unit within ministry; and list of national HPSR priorities.
Findings are presented narratively (and where applicable as percentages). We also used the data on published HPSR articles to plot a line chart to show the research volume in the EMR between 1 January 2010 and 31 December 2019 (Figure 1).
We conducted thematic analysis of the data generated from interviews. Two members of the research team conducted open coding to segregate the findings into chunks that relate to similar concepts. The emerging concepts were organised into themes and subthemes (taking into consideration the study objectives and interview guide). The identified themes were cross-checked and verified by the two members.
Ethics
The study was conducted following standard ethical guidelines and protocols for each country involved. The confidentiality and anonymity of responses were ensured at all times. Participation was voluntary and participants provided oral consent as part of the interview process. Interviews were digitally recorded after obtaining oral consent from interviewees; for those who refused to be recorded, extensive notetaking was used.
Results
The results section is divided into four parts, reflecting the different study objectives.
1. Amount and source of funding for health research and HPSR
a) Amount of funding for health research
Across the EMR countries (for which data was available), expenditure on R&D, as percentage of GDP, ranged from 0.02% (Syria and Sudan) to 1.3% (UAE), compared with the global average of 2.27% (2018).6 Although the absence of recent data on research expenditure for several EMR countries poses challenges for meaningful cross-comparison, publicly available data indicate that all EMR countries – with the exception of UAE – invest less than 1% of their GDP in R&D, despite larger shares of GDP for R&D being explicitly mentioned in the constitutions, laws or policies of some countries (e.g. Iran and Qatar). Expenditure on R&D was observed to increase with increasing income levels. Although spending on R&D was almost non-existent in low-income countries, it reached approximately 0.7% of GDP for Egypt and Morocco (both low-middle income) as well as Jordan (upper-middle income). High income countries (UAE, Qatar and Saudi Arabia) had higher rates of expenditure in addition to absolute value of funding for R&D (Table 1).
When looking at the percentage of health research expenditure out of total research expenditure and country GDP, the observation of an association between income levels and total value did not hold. Across EMR countries with publicly available data, Egypt (low-middle income) reported the highest percentage of health research expenditure out of total research expenditure (37%) and country GDP (0.27%). In the upper-middle income category, Jordan reported 23.4% and 0.01% for health research expenditure out of total research expenditure and country GDP, respectively. It was followed by Iraq, for which the values were 15% and 0.05% respectively. Among high-income countries, the highest absolute dollar values for health research expenditure were observed for Saudi Arabia and Qatar. However, the percentage of total research expenditure devoted to health research in these high-income countries was less than one-third of that seen in Egypt.
According to the WHO Consultative Expert Working Group on Research and Development, high-income countries should aim to commit 0.15–0.2% of their GDP to government-funded health research of all kinds, whereas low-middle income countries should aim to commit 0.05–0.1% of their GDP.7 None of the EMR countries in high-income groups for which data were available met or exceeded the target for high-income countries, while few middle-income countries, notably Iraq (0.05%, 2018) and Morocco (0.081%, 2013) met the target for their income groups.
b) Trend in research expenditure
Public investment in R&D (as a percentage of GDP) has increased significantly in Egypt and Saudi Arabia, while decreases have been noted in Iran, Tunisia and Sudan. There is also evidence of decreased expenditure in health research (out of total expenditure on research) in other countries (Iraq, Kuwait and Qatar) over time. In Iran, the set target of increasing spending on R&D (as a percentage of GDP) to 2.5% by 2015 was not met, which has been partially attributed to policy makers’ lack of belief in the return on investment in research.8 Similarly, Qatar failed to meet the government aim of spending 2.8% of GDP on R&D by 2015.9
Table 1. Overview of research funding landscape in the Eastern Mediterranean regiona
| R&D expenditure as percentage of GPD % (year) |
Absolute value of funding for research and development US$ (year) |
Absolute value of funding for health research US$ (year) |
Health research expenditure as percentage of R&D expenditure % (year) |
Health research expenditure as percentage of GDP % (year) |
|
| High-income countries | |||||
| Bahrain10,11 | 0.1 (2014) | $34 million (2014) | $2.3 million (2014) | 6.8 (2014) | 0.01 (2014) |
| Kuwait11 | 0.06 (2016) | $88 million (2018) | $0.03 million (2018) | 0.034 (2018) | 0.00002 (2018) |
| Qatar11 | 0.51 (2018) | $974 million (2018) | $147.5 million (2018) | 15 (2018) | 0.077 (2018) |
| Saudi Arabia11 | 0.82 (2013) | $6.1 billion (2013) | $693.8 million (2013) | 11 (2013) | 0.09 (2013) |
| United Arab Emirates6 | 1.3 (2018)3 | $5.4 billion (2018) | NA | NA | NA |
| Oman6,11 | 0.22 (2018) | $174 million (2018) | $17.03 million (2018) | 9.8 (2018) | 0.02 (2018) |
| Middle-income countries | |||||
| Iraq6,11 | 0.04 (2018) | $86 million (2017) | $15.06 million (2018) | 15 (2018)b | 0.05 (2018) |
| Iran6,8,12 | 0.83 (2017) | $3.7 billion (2017) | $117 million (2019) | 7.6 (2001)b | 0.03 (2019) |
| Jordan6,13 | 0.71 (2016) | $22.2 million (2020) | $ 5.2 million (2020) | 23 (2020) | 0.01 (2020) |
| Lebanon14 | 0.065 (2020) | $34 million (2020) | $0.7 million (2020) | 2.1 (2020) | 0.0013 (2020) |
| Libya | NA | NA | NA | NA | NA |
| Morocco15 | 0.71 (2010) | $662 million (2010) | $87.3 million (2013)1 | NA | 0.081% (2013) |
| Egypt16-18 | 0.74 (2019) | $3.8 billion (2020) | $132.7 million (2014) | 37 (2019) | 0.27 (2019) |
| Palestine6,16,18 | 0.49 (2013) | $7.6 million (2012) | NA | NA | NA |
| Pakistan6,11,19,20 | 0.24 (2017) | $ 730 million (2017) | $2.14 million (2001) | 7 (2000) | 0.002% (2001) |
| Tunisia6 | 0.6 (2018) | $23.9 million (2018) | NA | NA | NA |
| Low-income countries | |||||
| Djibouti | NA | NA | NA | NA | NA |
| Somalia21 | NA | NA | $12.44 million (2020) | 3.84% out of health sector budget (2020) | 0.21 (2020) |
| Sudan22 | 0.02 (study published in 2019) | $79.5 million (2005) | NA | NA | NA |
| Syria6 | 0.02 (2015) | $2 million (2015) | NA | NA | NA |
| Yemen | NA | NA | NA | NA | NA |
| Afghanistan | NA | NA | NA | NA | NA |
R&D = research and development; GDP = gross domestic product
a Table includes available information for each country; NA = data unavailable
b Most recent data available for R&D absolute value and health expenditure as percentage of R&D expenditure are from different years, so data is not comparable
Note: No data were available for any country on the absolute value of funding for health policy and systems research
c) Type of funded research
Reviews found that biomedical and clinical research dominated health research while HPSR and other social science research in healthcare remain undervalued and underfunded.23-25 It has also been suggested that existing funding bias toward biomedical and clinical research has created an imbalance in HPSR capacity development.23,26
It is worth noting that the documentation review did not retrieve information on how governments determine and allocate funding for R&D and health research to the different ministries, public universities, and national research council/institutes. There is also insufficient information on the process/criteria for funding allocation to different research fields/areas.
d) Funding sources for HPSR
Among the 22 EMR countries, none had explicit national funding or budget lines for HPSR in any of the published national agendas, government reports, national accounts, budget expenditure reports, central budget documents and ministerial reports audited as part of this review.
The funding sources for 1821 retrieved published articles on HPSR in the EMR (2010–2019) were analysed. A significant percentage of retrieved studies (n = 676, 37.1%) did not report any details on funding while 394 studies (21.6%) reported not being funded. A total of 751 (41.2%) were funded among which 144 (19.2%) reported more than one source of funding, bringing the total number of funders to 945. Results indicate that the most notable funding source among the total 945 funders was external/international grants (n = 430; 45.6%); followed by university/academia (n = 331; 35.1%) and government (n = 90; 9.5%). Regional entities funded only 4.6% of the included articles.
Several studies have highlighted the important role of international organisations and external donor resources in funding HPSR through project grants in the EMR.23,24 Although external donor resources are a potential source of HPSR funding, the capacity to develop strong proposals to compete for these funds is weak in the EMR, limiting opportunities to tap into international competitive funding opportunities for HPSR. For instance, in a cross-sectional survey of institutions undertaking health research in EMR countries, most institutions reported submitting less than 10 proposals to national, regional or international sources, and mainly in response to calls for proposals. Institutions received less than 10 grants regardless of funding source.27
At the regional level, the documentation review did not identify reliable data about total funding for HPSR-related projects. The WHO Regional Office is the main body offering funding support for health systems and HPSR projects on a regional level. Schemes offer small grants ranging between US$10 000 to US$15 000 per grant. The main beneficiaries of those grants have come from Egypt, Iran, Lebanon, Morocco, Pakistan, Somalia, Sudan and Yemen.9,28
2. HPSR production trend
Figure 1 details annual production of HPSR articles in EMR countries for 2010–2019 as found in the documentation review. Compared with 37 indexed articles obtained in 2010, a total of 348 indexed articles were obtained in 2019, indicating a 9.4-fold increase in publications. Results show that Iran was the country with the steadiest increase of production of HPSR articles. Iran’s leading position in HPSR production has been attributed to the establishment of the national scientific plan, which outlines the county’s vision and objectives for health research; national priority-setting exercises conducted to guide research themes; and the recent rise in number of research and academic centres which consequently led to a surge in qualified academics, researchers and advocates for HPSR.8,29 Egypt, Jordan, Saudi Arabia and Lebanon also showed progressive increases; Egypt experienced a slight decrease in publications in 2018. In Pakistan, there was a notable drop in publications in 2017 followed by a steady increase in 2018 and 2019. Several EMR countries experienced no major changes over the period.
Figure 1. Annual production of HPSR articles in the six countries with the highest number of publications in the Eastern Mediterranean region, 2010–2019a (click to enlarge)
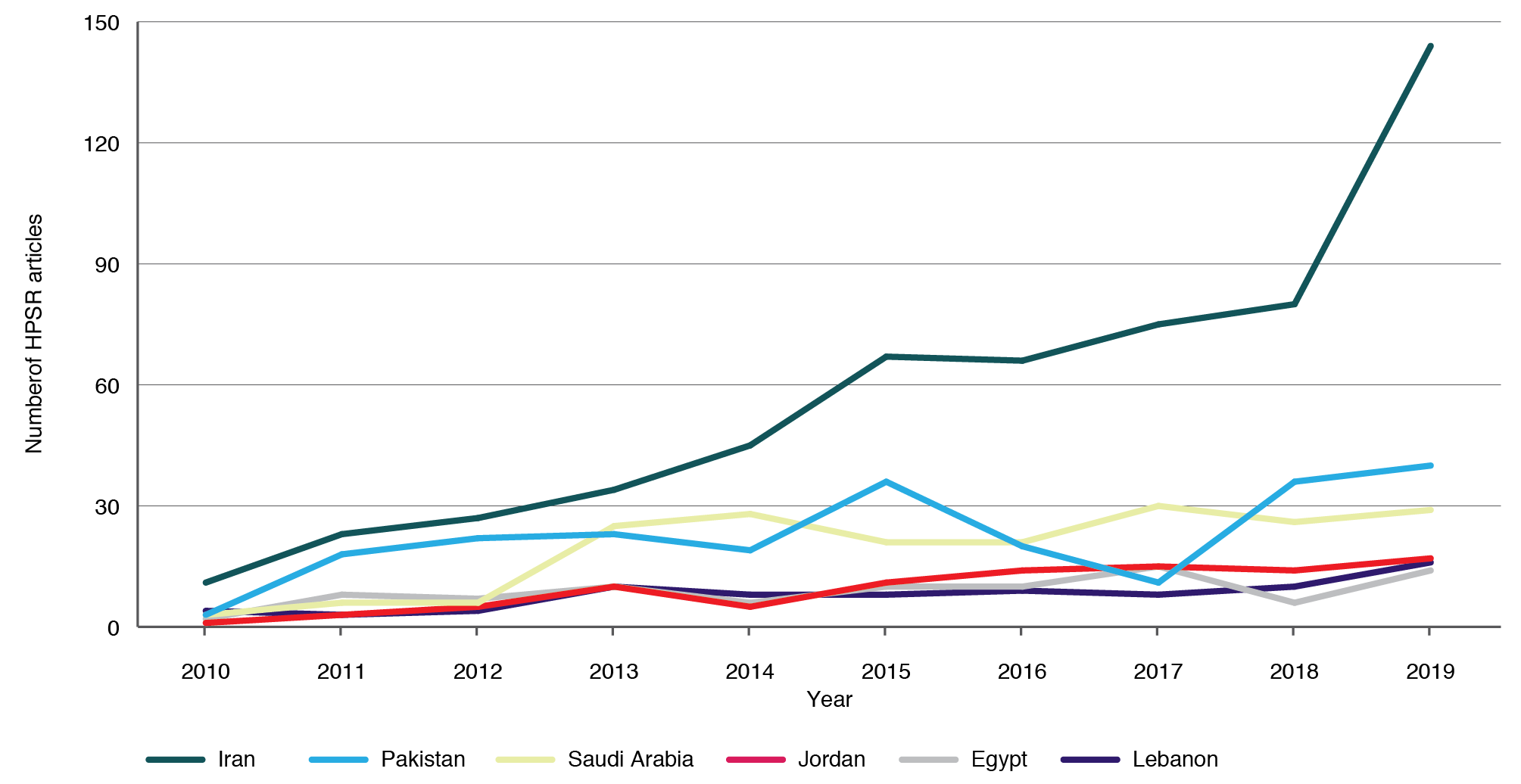
a Supplementary File 3 includes figure showing annual production of HPSR articles from all 22 countries (Available from: hdl.handle.net/10938/23237).
3. Presence of national research plans
Eleven EMR countries (Bahrain, Egypt, Iran, Jordan, Kuwait, Oman, Pakistan, Qatar, Saudi Arabia, Syria and Yemen) have a general national research strategy while nine others (Afghanistan, Iraq, Jordan, Oman, Pakistan, Qatar, Sudan, Tunisia, UAE) have a specific national health research plan, with only Iraq having a separate section within this plan dedicated for health systems research (see Supplementary File 4, available from: hdl.handle.net/10938/23237). In Bahrain, Lebanon, Saudi Arabia, Somalia and Yemen there is health research content in national health plans, health-sector reform strategies or national research plans, but this does not constitute a framework for a national health research policy nor a separate national health research plan. Notably, many countries were found to have a health research plan prepared by the Ministry of Health (MoH), but not a national research plan; this indicates that research is planned and conducted in a fragmented way in these countries with no wider vision at the national level. (For further details of the documentation review, see Supplementary File 1, available from: hdl.handle.net/10938/23237).
More than half the EMR countries have a national health research institute or council and/ or a health research promotion unit within the MoH that deals with and coordinates health research. In seven countries (Djibouti, Egypt, Jordan, Lebanon, Morocco, Oman and Tunisia), the health research responsibility and governance are located within a general research council, covering all fields of research and not just health.
On the other hand, only two countries in the EMR (Egypt and Oman) have a list of national HPSR priorities while four others (Iran, Iraq, Jordan and Yemen) include HPSR priorities as part of a larger list of national health research priorities.
4. Key factors influencing HPSR funding in the EMR
Findings from key informant interviews highlighted several factors that influence investment in or funding for HPSR in EMR countries. Key findings are presented below, categorised by broad themes:
Prevailing environment (political, economic and social pressures) and competing political interests
The continued political instability (e.g. in Lebanon and Sudan) and ongoing warfare (e.g. in Syria and Yemen) in the region have severely disrupted national research systems. Participants suggested that because of ongoing sociopolitical unrest in the region, government priorities had shifted towards defence and national security, while priorities of donors had shifted towards funding immediate emergency issues and humanitarian programs and services. This had limited the availability of funding for strengthening research, with repercussions for national health research systems. This was exacerbated by unstable government regimes in some countries which further impeded external and domestic funding for health research and HPSR. Participant comments included:
The government is going through a financial crisis… Actually I don’t think that research was a top priority in the government agenda due to different reasons, including their need to spend their available funds on emergency issues and salaries…. And charitable donations are more interested in emergencies and humanitarian aid.” (Palestine)
In 2020 alone, there were different epidemics: yellow fever, dengue, Rift valley, seasonal malaria and [coronavirus disease 2019] COVID-19 … with minimal budgets that are already spent on epidemics and disaster preparedness, how could there be funds for HPSR?” (Sudan)
Participants also highlighted political disinterest in supporting and funding HPSR since ‘research’ in general was not part of political platforms during elections. They felt that because of the interest in scoring political points, policy makers were more likely to prioritise funding of physically visible projects such as construction projects over research and HPSR, in particular where impact was not immediately visible.
Poor governance and stewardship of the national health research system
Although having a health research system is a precondition for establishing regulatory frameworks to drive HPSR activities, respondents highlighted the lack of a national policy or strategy for health research, or even a plan for sustainable funding that supported health research in several EMR countries. Where such plans did exist, interviewees suggested they lacked an explicit focus on HPSR. Furthermore, it was reported that existing governance systems were not conducive to building a favourable research climate because of extended health sector fragmentation and a multiplicity of national actors with conflicting agendas and demands. This had hindered both the effective alignment of health research priorities within the health sector agenda, and the institutionalisation of advancements in health research into national systems, they reported. Moreover, it was noted that most EMR countries lacked formal priority setting to shape the health research agenda and set HPSR priorities. This situation was exacerbated by limited networking among research entities performing HPSR and the absence of an independent governing body that promotes HPSR. As stated by participants:
Research efforts are generally not well coordinated in the country and there is no adequate government oversight to ensure efficiency in using resources… there are many duplications and dichotomies that adversely affect the already meagre funding for research. (Sudan)
Everyone is working alone as there is a cultural mentality of competition. It is a major problem that could be tackled by a strong leadership, which doesn’t exist for the moment. (Palestine)
Influence of external funders and poor alignment with national priorities
EMR countries’ strong dependence on international funding came at the expense of addressing national health system priorities and local community needs, participants suggested. External funding agencies set research topics which often did not align with national priorities, despite the presence of national research plans in several EMR countries. As stated by participants:
This is creating a missed opportunity to demonstrate the value of HPSR since it [HPSR] is not being used to influence policies, yet, the main purpose of HPSR is to influence decision-making. (Iran)
We are a donor-dependent and donor-driven country. The smart thing is how to merge our own needs with the donor interests. (Palestine)
Limited domestic commitments, poor accountability and lack of explicit funding allocation criteria
There was consensus among participants concerning insufficient funding for health research in general and the lack of explicit funding or budget lines for HPSR. Participants also noted the absence of clearly defined processes to allocate national budgets for research, with no specific criteria or formula to guide funding allocation. Because budget allocation is likely to be based on preferences of authorities, the lack of familiarity with the HPSR concept and limited awareness on its importance affected the total budget dedicated to HPSR. Participants also highlighted the lack of accountability mechanisms to track spending on health research. According to participants:
Since there is no specific rule for allocating budgets to various research areas, budget allocation is more based on the preferences of the authorities. When the authority is not familiar with the HPSR concept or does not consider it important, he may not allocate budget to this area. (Iran)
The [R&D] budget at the national level represents a merely technical bureaucratic numerical allocation for resources…the budget items are historical budget … we don’t have specific criteria or formula to guide allocation decisions and there is no accountability for spending on research at the national or institutional level. (Lebanon)
Additionally, participants noted that the lack of a national entity for funding HPSR further contributed to the weak sustainability and transparency in budget allocation for such research. For instance, it was mentioned that funding acquired for HPSR (if any) was often used for other services and expenses, including health program delivery and salaries of staff. According to one participant:
Whenever the need to cut down on [government] budget arises, the research line was the first to be affected, making it the weakest link. (Lebanon)
Poor understanding of HPSR and a preference for biomedical and clinical research
There was consensus among participants that the concept of the health research system and HPSR was largely misunderstood and thus underappreciated in the EMR. Moreover, there was a clear lack of awareness and recognition of its role in strengthening health systems, achieving universal healthcare and promoting population health. Governmental bodies did not consider HPSR as an essential component to support policy, but rather perceived it as a “luxury”, as reflected by a weak political will to support and fund HPSR.
Resources are limited but the main problem is that decision-makers don’t see its importance. (Palestine)
Furthermore, even when governments and private national donor agencies showed interest in allocating funds for health research, they mainly targeted biomedical and clinical research where results could be easily applied for the development of new diagnostic and treatment options, participants suggested, as illustrated below:
Biomedical research receives high levels of funding because of high demand for this kind of research…results are usually visible and could be easily applied… and we have large number of health care providers and researchers in this area. (Egypt)
It was also noted that researchers in universities and major research institutes concentrated mainly on clinical and biomedical topics that were of academic interest and publishable in high-impact journals, which could advance their careers.
Weak research culture and climate for evidence-informed decision making
Increases in domestic funding commitments are difficult to achieve without stronger policy maker demand for HPSR. Although the usefulness of HPSR derives directly from its ability to inform policy and decision making, participants highlighted that HPSR was not being used to influence policies, or was being used only to a limited extent with no institutionalised mechanism for using research results in policy or decision making. According to policy maker interviewees, there were poor incentives to promote the use of research evidence in decision making and no mandates or accountability mechanisms to use research evidence as an input in decision making. Additional insights are provided below:
Rather than looking for evidence to make decisions based on it, decisions are made based on the mindsets of the managers, and sometimes researchers are even asked to find evidence to support the managers’ decisions. (Iran)
There are several barriers for incorporating research evidence into policy and decision making in Sudan…one major aspect is the prevailing culture of decision making that undervalues evidence; another dimension is lack of effective relationships between researchers and policy makers; there is also lack of platforms and vehicles for research dissemination. (Sudan)
At the level of research/academia, researchers were incentivised to publish in peer-reviewed journals but there were no institutional mechanisms to promote their work for use in evidence-informed policy making. Although some initiatives were being undertaken to promote HPSR, these were ad hoc, project based, and insufficient to make systemic changes to the prevailing research culture. There was unanimous agreement that the research culture needed to be changed at the policy, academia/researchers and funding organisations levels.
Insufficient infrastructure and human resources to support HPSR
Participants acknowledged the limited number of HPSR researchers and universities that have stand-alone HPSR programs and therefore low capacity to produce and translate evidence from HPSR to inform policy decisions. As highlighted by one participant:
Even if there is a budget allocated for it, HPSR cannot be conducted without the basic prerequisites like specialised human resources. (Lebanon)
Discussion
To our knowledge, this is the first study to assess HPSR funding including key determinants and prevailing attitudes in the EMR.
Despite the regional disparities between study countries in terms of socioeconomic levels, strength of health systems and political stability, the study findings reveal that the national funding for R&D in general, and for health research specifically, has been low in comparative terms and lagging behind at the global scale, while funding for HPSR on a national level has been lacking. Among the 22 EMR countries, none had explicit national funding or a budget line for HPSR. Analysis of funding sources for published HPSR studies in the region showed that the most notable funding source was external/international grants followed by university/academia and then government. Nonetheless, the dependence of the EMR on international funding comes at the expense of addressing health system priorities, which may threaten sustainability and national ownership of HPSR.
Although our findings indicate that HPSR publications have increased over time, this still falls short of the scale of research that is needed for strengthening health systems and informing current transformations in the region. More efforts are needed to align HPSR production and translation with demand for evidence from policy making.27
A number of factors have been identified as influencing investment in or funding for health research in general and HPSR in the region. The under-investment in health research on a national level across the EMR has given rise to critical skills shortages, weak capacity and comparatively low research productivity.28
Moving forward, governments in the EMR are urged to establish or revise their national health research strategies and prioritise HPSR while ensuring required governance, resources and infrastructure are in place. Formal participation by all stakeholders in the development of the strategy could enhance the legitimacy of the process and facilitate implementation. Governments could also consider forming a separate institute or structure for HPSR that would enable better governance of HPSR activities aligned with the national health strategy. Additionally, governments are urged to increase domestic funding for HPSR, to reduce reliance on external donors while improving the focus of HPSR on national priorities.
An explicit national funding or budget line for HPSR should be established with sustainable and transparent processes in place for mobilising, allocating and tracking funds for HPSR and health research in general. Because funding from international sources will continue to play a role in the region, strong governance to ensure coordinated efforts and alignment to country priorities is key to attaining maximum return on investment. Furthermore, investing in strengthening capacity and raising awareness for HPSR is needed to improve the prevailing culture for research and evidence-informed decision making. Individual-level capacity should be complemented by institutional-level mechanisms and policies for using research evidence to support decision making and to hold decision makers accountable for their decisions. Incentive systems to promote knowledge translation work and interdisciplinary research can also incentivise researchers to engage in HPSR.
At the regional level, considerations could be given to establishing a regional strategy which articulates the vision, goals and priorities for HPSR in the region, as well as guiding resource mobilisation and allocation decisions. This could also help inform country-level strategies and funding for HPSR. A regional advocacy coalition could also be formed to raise regional funds for HPSR in the EMR.
Conclusion
Although many of the region’s policy priorities are related to health systems30, study findings reveal that the overall investment in health research generally and HPSR in particular is still low, with limited recognition of the importance of HPSR in countries of the EMR. Regional and national strategies are needed to address this shortfall, with increased investment in HPSR vital to strengthening health systems across the region.
Acknowledgements
This work was supported by the Alliance for Health Policy and Systems Research, World Health Organization. The authors are themselves alone responsible for the views expressed in the article. This article does not represent the views, decisions, or policies of the Alliance for Health Policy and Systems Research.
Appreciation is extended to country teams and authors for conducting the work in a short time. Thanks are extended to: Egypt – Drs Mahmoud Sakr, Sameh Sororur and Mohamed Ramadan; Iran – Drs Zhaleh Abdi, Sahand Riazi-Isfahani, supervised by Dr Ali Akbari Sari; Palestine – Dr Elias Boutaher of Juzoor; Sudan – Dr Lamis Beshir; and Dr Radwa Mekky from MENA HPF. We would also like to acknowledge Diana Jamal, Mathilda Jabbour, Najla Daher, Aya Harb and Sahar Nassour from the American University of Beirut, Lebanon for their support in conducting the regional analysis.
Peer review and provenance
Externally peer reviewed, invited.
Copyright: 
© 2021 El Rabbat et al. This article is licensed under a Creative Commons Attribution 3.0 IGO Licence, which allows others to redistribute, adapt and share this work for any purpose provided they attribute the work and indicate if changes were made. See: https://creativecommons.org/licenses/by/3.0/igo/
References
- 1. Langlois ÉV, Daniels K, Akl EA. Evidence synthesis for health policy and systems: a methods guide. Geneva: WHO; 2018 [cited 2021 Oct 13]. Available from: www.who.int/alliance-hpsr/resources/publications/Alliance-evidence-synthesis-MethodsGuide.pdf
- 2. Sheikh K, Gilson L, Agyepong IA, Hanson K, Ssengooba F, Bennett S. Building the field of health policy and systems research: framing the questions. PLoS Med. 2011;8(8):e1001073. CrossRef | PubMed
- 3. Gilson L, Hanson K, Sheikh K, Agyepong IA, Ssengooba F, Bennett S. Building the field of health policy and systems research: social science matters. PLoS Med. 2011;8(8):e1001079. CrossRef | PubMed
- 4. Grépin KA, Pinkstaff CB, Shroff ZC, Ghaffar A. Donor funding health policy and systems research in low- and middle-income countries: how much, from where and to whom. Health Res Policy Syst. 2017;15(1):68. CrossRef | PubMed
- 5. Bennett S, Agyepong IA, Sheikh K, Hanson K, Ssengooba F, Gilson L. Building the field of health policy and systems research: an agenda for action. PLoS medicine. 2011;8(8):e1001081. CrossRef | PubMed
- 6. World Bank Data Portal. Research and development expenditure (% of GDP). Washington, DC: The World Bank; 2021 [cited 2021 Nov 3]. Available from: data.worldbank.org/indicator/GB.XPD.RSDV.GD.ZS
- 7. World Health Organization. Research and development to meet health needs in developing countries: strengthening global financing and coordination. Report of the consultative expert working group on research and development: financing and coordination. Geneva: WHO; 2012 [cited 2021 Nov 1]. Available from: apps.who.int/iris/handle/10665/254706
- 8. Mansoori P. Evolution of Iran’s health research system over the past 50 years: a narrative review. J Global Health. 2018;8(2):020703. CrossRef | PubMed
- 9. Shideed O, Al Gasseer N. Appraisal of the research grant schemes of the World Health Organization Regional Office for the Eastern Mediterranean: the way forward. East Mediterr Health J. 2012;18 (5):515–21. CrossRef | PubMed
- 10. UNESCO Institute for Statistics. Science, technology and innovation: gross domestic expenditure on R&D (GERD), GERD as a percentage of GDP, GERD per capita and GERD per researcher. Canada: UNESCO; 2020 [cited 2021, Nov 3]. Available from: data.uis.unesco.org/?queryid=74
- 11. World Health Organization. Global Observatory on Health R&D, gross domestic R&D expenditure on health (health GERD) as a % of gross domestic product (GDP). 2020 [cited 2021 Nov 1]. Available from: www.who.int/observatories/global-observatory-on-health-research-and-development/indicators/gross-domestic-r-d-expenditure-on-health-as-a-percent-of-gross-domestic-product
- 12. The World Bank. Islamic Republic of Iran. Washington DC; The World Bank; 2021 [cited 2021 Nov 1]. Available from: www.worldbank.org/en/country/iran/overview#1
- 13. Ministry of Finance General Budget Department. The general budget law for the fiscal year 2020. Jordan: Ministry of Finance; 2020 [cited 2021 Nov 3]. Available in Arabic from: www.gbd.gov.jo/Uploads/Files/speechs/ar/2020.pdf
- 14. Annual Budget Document. The general budget and attached budgets. Lebanon: Ministry of Finance; 2020 [cited 2021 Nov 3]. Available in Arabic from: www.finance.gov.lb/en-us/Finance/BI/ABDP/Annual%20Budget%20Documents%20and%20Process/Budget%20%20Law%202020.pdf
- 15. Ministry of Health. National Health Accounts. Morocco: Ministry of Health Morocco; 2015 [cited 2021 Nov 3]. Available in French from: www.sante.gov.ma/Publications/Etudes_enquete/Documents/Comptes%20Nationaux%20de%20la%20Sant%C3%A9%20Rapport%202015.pdf
- 16. Ministry of Finance Egypt. General framework of the draft state budget for the fiscal year 2019/2020. Egypt: Ministry of Finance; 2020 [cited 2021 Nov 1]. Available from: www.mof.gov.eg/en/posts/stateGeneralBudget/601bdca48e87100007469676/2019-2020%20General%20Budget
- 17. Egypt Today. Egypt’s health sector accounts for LE 258B of 20/21 spending allocations. 2020. Egypt: Egypt Today; 2020 April 21 [cited 2021 Nov 1]. Available from: www.egypttoday.com/Article/3/84958/Egypt%E2%80%99s-health-sector-accounts-for-LE-258B-of-20-21
- 18. Qumsiyeh M, Isaac J. Research and development in the Occupied Palestinian Territories: challenges and opportunities. Arab Studies Quarterly. 2012;34(3):158–72. Article
- 19. Akhtar T, Khan J. Health research capacity in Pakistan. Pakistan: Council on Health Research for Development; 2000 [cited 2021 Nov 3]. Available from: www.cohred.org/downloads/681.pdf
- 20. Shakeel H, Khan N. Innovations in Pakistani Universities, R&D centres and corporate research institutes. Development. 2008;5:1981–90. Article
- 21. World Health Organization. Strategic review of the Somali health sector: challenges and prioritized actions. Geneva: WHO; 2015 [cited 2021 Oct 13]. Available from: www.somalimedicalarchives.org/media/attachments/2021/09/18/hss-review-2015.pdf
- 22. Bannaga TEJ, Mohammed AI. Situation of scientific research in Sudan public universities. East African Scholars J Edu Humanit Lit. 2019;2(3)191–6. Article
- 23. AlKhaldi M, Al-Surimi K, Meghari H. Health policy and systems research in the Arab world: concepts, evolution, challenges, and application necessity for COVID-19 pandemic and beyond. In: Laher I, editor. Handbook of Healthcare in the Arab World. Switzerland: Springer International Publishing; 2020. CrossRef
- 24. Mandil A, El Jardali F, El Feky S, Nour M, Al Abbar M, Bou Karroum L. Health research institutional mapping: an Eastern Mediterranean Regional perspective. East Mediterr Health J. 2018;24(02):189–97. CrossRef | PubMed
- 25. Tadmouri GO, Mandil A, Rashidian A. Biomedical and health research geography in the Eastern Mediterranean Region. East Mediterr Health J. 2019;25(10):728–43. CrossRef | PubMed
- 26. Cairney P, Oliver K. Evidence-based policymaking is not like evidence-based medicine, so how far should you go to bridge the divide between evidence and policy? Health Res Policy Syst. 2017;15(1):1–11. CrossRef | PubMed
- 27. El-Jardali F, Mandil A, Jamal D, BouKarroum L, El-Feky S, Nour M, et al. Engagement of health research institutions in knowledge translation in the Eastern Mediterranean Region. East Mediterr Health J. 2018;24(7). CrossRef | PubMed
- 28. Ismail SA, McDonald A, Dubois E, Aljohani FG, Coutts AP, Majeed A, et al. Assessing the state of health research in the Eastern Mediterranean Region. J R Soc Med. 2013;106(6):224–33. CrossRef | PubMed
- 29. World Health Organization. Health Evidence Network Synthesis Report 69: what is the evidence on policies, interventions and tools for establishing and/or strengthening national health research systems and their effectiveness? Copenhagen: WHO Regional Office for Europe; 2020 [cited 2021 Nov 1]. Available from: apps.who.int/iris/bitstream/handle/10665/331703/9789289054942-eng.pdf
- 30. El-Jardali F, Makhoul J, Jamal D, Ranson MK, Kronfol NM, Tchaghchagian V. Eliciting policymakers’ and stakeholders’ opinions to help shape health system research priorities in the Middle East and North Africa region. Health Policy Plan. 2010;25(1):15–27. CrossRef | PubMed