Abstract
Objectives and importance of study: Colorectal cancer (CRC) is Australia’s fourth most commonly diagnosed cancer. CRC screening is an effective intervention to reduce this burden. The National Bowel Cancer Screening Program (NBCSP) provides 2-yearly immunochemical faecal occult blood tests (iFOBTs) to Australians aged 50–74 years; a diagnostic colonoscopy is conducted after a positive iFOBT. Clinical guidelines inform colonoscopy usage, and appropriate use of these guidelines is vital to investigate gastrointestinal symptoms, detect bowel abnormalities and CRC, and remove precancerous polyps.
Colonoscopy services are under strain, with limited formal strategies to prioritise patients. There are concerns among practitioners and patient advocates that the NBCSP generates additional colonoscopy requests and increases wait times, worsening patient outcomes and prolonging distress. In this research study, we estimate and project colonoscopy use in Australia from 2001 to 2030 and determine the impact of the NBCSP by examining model-estimated NBCSP colonoscopy demand.
Methods: Colonoscopy use in Australia was compiled using Medicare Benefits Schedule (MBS) claims for colonoscopies from 2001 to 2019. From these data, projections were made from 2020 to 2030. Policy1-Bowel, a microsimulation model, was used to estimate NBCSP-related colonoscopy demand from screening follow-up and colonoscopic surveillance from 2006 to 2030.
Results: MBS-funded colonoscopy use increased from 284 676 in 2001 to 663 213 in 2019. Annual use is projected to be more than 780 000 by 2030. Of these, 10–14% are projected to be generated by the NBCSP. Per-capita MBS-funded colonoscopy utilisation increased 0.2% annually over 2015–2019, a slowing of growth compared to previous trends.
Conclusion: The NBCSP accounts for a modest fraction of colonoscopy use in Australia, and a better understanding of colonoscopy use not associated with the NBCSP is needed. Promoting adherence to guideline-recommended iFOBT and colonoscopy use could ease pressure on services and improve outcomes.
Full text
Introduction
Colorectal cancer (CRC) is the fourth most commonly diagnosed cancer and second most common cause of cancer death in Australia, with an estimated 15 632 cases and 5363 deaths from CRC in 2020.1 The health and financial burden for both individuals and the health system is high – excess costs to the health system can be up to $82 117 per CRC patient annually, with variations by stage and time since diagnosis.2 Additionally, CRC incidence rates have increased significantly for people under 50 years of age during recent decades3, raising concern about the future burden on the health system.
CRC screening can be highly effective in decreasing CRC incidence through the detection and removal of precancerous polyps and reducing CRC mortality through early detection and treatment. A key sequela of screening is colonoscopy referral, via which precancerous polyps can be detected and removed; this can prevent cancers or detect them at earlier stages, leading to higher survival rates.4 Although colonoscopies can be a primary screening tool for individuals at higher risk of developing CRC, individuals with an average risk of CRC are recommended to screen using the immunochemical faecal occult blood test (iFOBT). For the average-risk population, iFOBT screening is more cost-effective, less invasive and safer than a colonoscopy.5
In Australia, the National Bowel Cancer Screening Program (NBCSP) provides iFOBT screening to all individuals aged 50–74 years every 2 years. The program began in 2006; initially, it was offered to only a small number of age groups, but a full rollout was achieved from 2019. A previous analysis showed that NBCSP-recommended iFOBT is favourable and cost-effective for the average-risk Australian population compared with colonoscopy as primary screening.5 General practitioners (GPs) and other groups outside the NBCSP can also distribute iFOBT tests. The 2017 National Health and Medical Research Council–approved clinical practice guidelines for early detection and management of CRC recommend colonoscopy for follow-up to a positive iFOBT, surveillance of individuals with past CRC or polyps, or primary screening of individuals with a moderately increased risk of CRC from family history.6 The Colonoscopy Clinical Care Standard prescribes appropriate use and delivery of colonoscopy. Currently, there is a significant shortfall in real-world patient experience, with one-third of patients waiting longer than recommended for follow-up treatment after indications for possible CRC.7 In addition to their role in CRC screening, colonoscopies are also indicated for diagnosing symptomatic patients, such as those presenting with rectal bleeding; blood, pus or mucus in faecal matter; or other changes in bowel habits.6
Colonoscopy services are under increasing strain, and there has been concern that the NBCSP may increase demand on an already overtaxed system.8 Previous research has estimated that the NBCSP will generate more than 100 000 colonoscopies annually from 2020.9 In 2019, just over 660 000 colonoscopies were subsidised through the Medicare Benefits Schedule (MBS), constituting an estimated 80% of the total colonoscopies in Australia; the remaining 20% were available through state-funded hospital services.10,11 The Australian health system has a finite colonoscopy capacity, and long wait times resulting from excess demand have been documented; diagnostic colonoscopies are recommended to be delivered within 180 days.12 Colonoscopies are invasive and associated with a risk of complications requiring hospitalisation.13 Their use should therefore be based on clinical guidelines and prioritised for those at greatest risk. Concerns about potential increases in colonoscopy demand are exacerbated by variations in demand by certain demographic groups, and unexpected external pressures on the health system and its capacity to deliver timely colonoscopies, such as disruptions caused by the COVID-19 pandemic. These variations may exacerbate existing health inequities.7,14
To better understand the future impact of the NBCSP on colonoscopy services and guide prioritisation efforts, this analysis aims to use existing data on colonoscopy use to project the total number of MBS-funded colonoscopies. It also aims to determine the impact of the NBCSP by estimating the number of colonoscopies generated by referrals from the NBCSP, including diagnostic and surveillance colonoscopies.
Methods
MBS-funded colonoscopy use in Australia
We used publicly available data to extract the reported number of colonoscopies from 2001 to 2020 from Medicare statistics, stratified by quarter and state/territory.11 The MBS item codes included are shown in Supplementary Table 1 (available from: figshare.com/articles/dataset/Worthington_et_al_PHRP_2022_Supplementary_Tables_xlsx/21579570). The 2020 data were a significant outlier due to the effect of the COVID-19 pandemic.14,15
The linear trend was calculated using least squares linear regression based on the data from 2015–2019, as these data represent recent trends in use after the full rollout of the NBCSP. This was used to project MBS-recorded colonoscopy use for 2021–2030. As noted above, the 2020 data were an outlier and so were excluded from the regression training set. The 95% prediction interval (the statistically likely probable range of slopes for the linear fit), which generates the 95% confidence interval for each year, was also calculated. Australian population data and projections from the Australian Bureau of Statistics (ABS) were used to calculate colonoscopy numbers and rates per 100 000 Australians.16,17 These population projections allow the modelling to capture the effects of a growing and ageing population, which will contribute to an increase in colonoscopies and CRC. Similar estimates were used for state populations.17
Model-estimated program-related colonoscopy use
We used Policy1-Bowel, a calibrated and validated microsimulation model of CRC development in individuals for the Australian population, to estimate the number of colonoscopies attributable to the NBCSP.9 Policy1- Bowel models individuals in Australia, including their precancer natural history; screening behaviours; and CRC diagnosis, treatment and survival. This includes both index colonoscopies (diagnostic colonoscopies to follow up a positive iFOBT test) and surveillance colonoscopies (further colonoscopies recommended after an individual has a polyp detected at index colonoscopy); colonoscopies after a bowel resection were not modelled.
Policy1-Bowel simulates the development of CRC in millions of men and women, including both the conventional adenoma and serrated lesion pathways. This natural history simulation was calibrated to reproduce CRC in Australia. Overlaid with this was a simulation of the NBCSP, including the phased rollout from 2006 to 2019 and detailed modelling of screening participation dependent on an individual’s age, sex and previous participation in the NBCSP. All index and surveillance colonoscopies were modelled; surveillance recommendations were modelled according to guidelines, including previous guidelines up to 2018 and updated guidelines from 2019.18,19 This model has previously been used to inform CRC screening and colonoscopy surveillance guidelines in Australia, among other evaluations. Full technical details have been published previously.9
A key assumption for this study is the adherence rate to diagnostic colonoscopy after a positive iFOBT and surveillance colonoscopies after polypectomy. For diagnostic colonoscopies, the adherence rate after positive iFOBT is modelled at 66%, with age- and sex-specific rates ranging from 65 to 76%, based on nationwide rates observed in 2017–18.7
If a precancerous neoplasia is found at index colonoscopy, an individual is referred for subsequent surveillance colonoscopies at an interval determined by the 2019 clinical practice guidelines for surveillance.19 For individuals with a small adenoma only, a 10-yearly interval is recommended before the next surveillance; if a more serious neoplasia is found, individuals can be recommended another colonoscopy after a year. An 80% compliance rate is assumed for surveillance colonoscopies, consistent with previous modelling.9 Additionally, surveillance colonoscopies were assumed to cease at age 75 – any colonoscopies past this age were not considered to be program related. Overall participation in NBCSP screening was modelled at 42.4%, as observed in 2017–18. This participation rate was assumed to remain constant in future years7; it varied by age, sex, state or territory and previous program participation. Data from the monitoring reports on diagnostic colonoscopy rates by healthcare provider setting (private versus public) were used to estimate the range of NBCSP-generated colonoscopies funded through the MBS.7
Additional analysis
The Australian Government target for NBCSP participation is 56.6%.20 As a supplementary analysis, we estimated colonoscopy use if participation increased to 56.6% from 2023.
Adherence to index colonoscopies is currently reported to be 66%.7 However, this is likely an underestimate due to incomplete reporting. Therefore, we simulated the NBCSP with index colonoscopy compliance modelled at 80% from 2006.
It is known that colonoscopy surveillance schedules can vary in practice from current guideline recommendations at clinician discretion.21 However, there is insufficient evidence to quantify adherence to the new guidelines. To capture this, we simulated the expected colonoscopy use using the pre-201818 guidelines indefinitely.
Results
Historical data and projections
MBS-reimbursed colonoscopies from 2001 to 2020 in Australia are shown in Table 1. Table 1 also shows the linear projection of colonoscopies from 2021 to 2030. Additional estimates have been generated from 2031 to 2050, with the caveat that these estimates come with a high degree of uncertainty. For the trends over 2015–2019, the R-squared value of the linear fit was 95%, indicating a very good fit. The reported and projected data are shown in Figure 1. These results are also presented per 100 000 people, using ABS population projections. The 95% prediction intervals for each year are also shown in Figure 1.
Numbers of MBS-funded colonoscopies increased from 284 676 (1477 per 100 000 people) in 2001 to 663 213 (2615 per 100 000 people) in 2019. Based on the linear trends, we estimated that the number of publicly funded colonoscopies in 2030 would be 789 350 (95% confidence interval [CI] 727 298, 851 402), or 2637 per 100 000 (95% CI 2430, 2844), and the year-on-year colonoscopy per-capita increase was estimated to be a constant 0.18% (95% CI –0.17, 0.44%).
Reported and projected data are shown by state and territory in Supplementary Table 3 (available from figshare.com/articles/dataset/Worthington_et_al_PHRP_2022_Supplementary_Tables_xlsx/21579570), including average use per capita.
Modelled estimates
The outcomes for NBCSP-related colonoscopies as estimated by Policy1-Bowel are shown alongside the MBS estimates in Table 1 and Figure 1. In 2017–18,7 72.1% of reported NBCSP-generated colonoscopies were performed through the private health system, 17.5% were performed through the public health system, and 10.4% were not stated. Since colonoscopies performed by private providers would be recorded by the MBS but public colonoscopies may not, we estimated that 72.1–100% of NBCSP-generated colonoscopies were MBS recorded. This is also presented in Table 1.
Figure 1. MBS-reported colonoscopy use, 2001–2020, estimated colonoscopy demand 2019–2030 and the upper and lower bounds of the 95% prediction interval, and model-estimated NBCSP-related colonoscopy demand; shown as a total (top) and per 100 000 people (bottom) (click to enlarge)
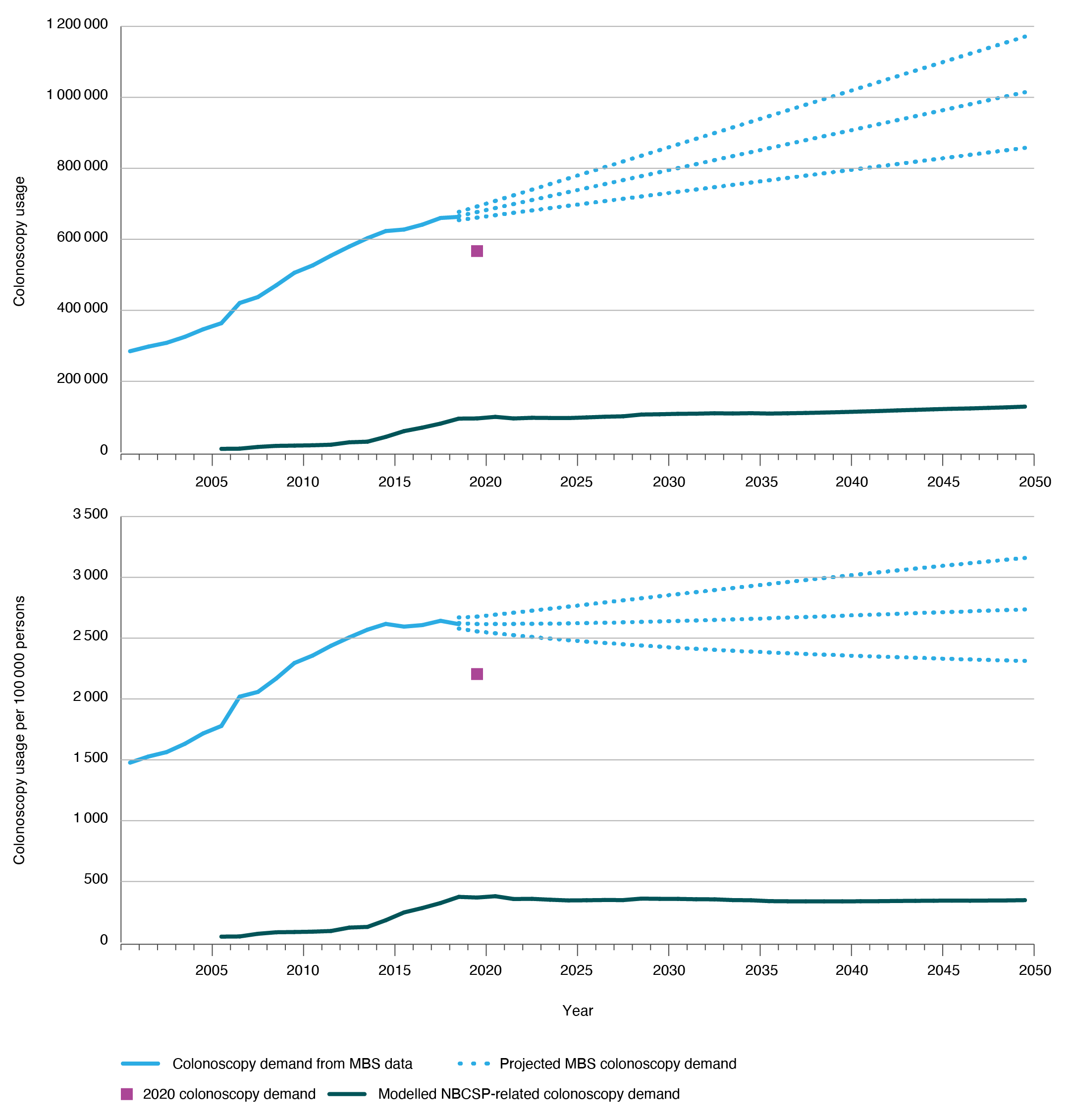
Note: Estimates for years after 2030 are subject to significant uncertainty and included as qualitative estimates
Table 1. MBS data on colonoscopy use in Australia, as a total and per 100 000 people alive, and statistical projections for future total colonoscopy use
| Year | Total (Australia) | Per 100 000 people alive | ||||||||
| MBS | NBCSP | NBCSP % of MBSa | Index colonoscopies
(% of NBCSP) |
Surveillance colonoscopies (% of NBCSP) | MBS | NBCSP | Index colonoscopies | Surveillance colonoscopies | ||
| Historical MBS data | 2001 | 284,676 | 0 | 0 | 0 (0) | 0 (0) | 1,477.1 | 0.0 | 0.0 | 0.0 |
| 2002 | 297,683 | 0 | 0 | 0 (0) | 0 (0) | 1 527.1 | 0.0 | 0.0 | 0.0 | |
| 2003 | 308,361 | 0 | 0 | 0 (0) | 0 (0) | 1,563.8 | 0.0 | 0.0 | 0.0 | |
| 2004 | 325,246 | 0 | 0 | 0 (0) | 0 (0) | 1,631.9 | 0.0 | 0.0 | 0.0 | |
| 2005 | 346,415 | 0 | 0 | 0 (0) | 0 (0) | 1,717.1 | 0.0 | 0.0 | 0.0 | |
| 2006 | 363,687 | 9,641 | 2–3 | 9 641 (100) | 0 (0) | 1,778.5 | 47.1 | 47.1 | 0.0 | |
| 2007 | 420,528 | 10,155 | 2 | 9 967 (98) | 188 (2) | 2,019.3 | 48.8 | 47.9 | 0.9 | |
| 2008 | 437,295 | 15,003 | 2–3 | 14 799 (99) | 204 (1) | 2,058.2 | 70.6 | 69.7 | 1.0 | |
| 2009 | 470,291 | 18,004 | 3–4 | 15 531 (86) | 2,472 (14) | 2,168.4 | 83.0 | 71.6 | 11.4 | |
| 2010 | 505,738 | 18,766 | 3–4 | 16 019 (85) | 2,748 (15) | 2,295.8 | 85.2 | 72.7 | 12.5 | |
| 2011 | 526,567 | 19,651 | 3–4 | 14 956 (76) | 4,694 (24) | 2,357.4 | 88.0 | 67.0 | 21.0 | |
| 2012 | 553,994 | 21,259 | 3–4 | 15 379 (72) | 5,881 (28) | 2,437.2 | 93.5 | 67.7 | 25.9 | |
| 2013 | 579,536 | 28,052 | 3–5 | 21 349 (76) | 6,703 (24) | 2,506.1 | 121.3 | 92.3 | 29.0 | |
| 2014 | 603,205 | 29 854 | 4–5 | 22 047 (74) | 7,808 (26) | 2,569.8 | 127.2 | 93.9 | 33.3 | |
| 2015 | 623,205 | 43 313 | 5–7 | 35 039 (81) | 8 274 (19) | 2,617.1 | 181.9 | 147.1 | 34.7 | |
| 2016 | 627,585 | 59 514 | 7–9 | 48 789 (82) | 10 725 (18) | 2,594.8 | 246.1 | 201.7 | 44.3 | |
| 2017 | 641,323 | 69 403 | 8–11 | 57 608 (83) | 11 795 (17) | 2,607.3 | 282.2 | 234.2 | 48.0 | |
| 2018 | 660,083 | 80 748 | 9–12 | 65 751 (81) | 14 997 (19) | 2,642.7 | 323.3 | 263.2 | 60.0 | |
| 2019 | 663,213 | 94 809 | 10–14 | 74 663 (79) | 20 146 (21) | 2,615.1 | 373.8 | 294.4 | 79.4 | |
| 2020 | 568,439 | 95 328b | 12–17 | 74 954 (79) | 20 374 (21) | 2,213.3 | 371.2 | 291.9 | 79.3 | |
| Projections based on 2015–2019 data | 2021 | 688,087 | 99,731 | 10–14 | 75,114 (75) | 24,618 (25) | 2,632.9 | 379.3 | 285.6 | 93.6 |
| 2022 | 699,339 | 95,241 | 10–14 | 75,083 (79) | 20,157 (21) | 2,637.3 | 356.4 | 281.0 | 75.4 | |
| 2023 | 710,590 | 97 ,092 | 10–14 | 74,913 (77) | 22,180 (23) | 2,641.7 | 357.7 | 276.0 | 81.7 | |
| 2024 | 721,842 | 96,600 | 10–13 | 75,284 (78) | 21,316 (22) | 2,646.1 | 350.5 | 273.2 | 77.4 | |
| 2025 | 733,093 | 96,364 | 9–13 | 75,512 (78) | 20,852 (22) | 2,650.5 | 344.6 | 270.0 | 74.6 | |
| 2026 | 744,344 | 98,178 | 10–13 | 75 924 (77) | 22 255 (23) | 2,654.9 | 346.1 | 267.6 | 78.5 | |
| 2027 | 755,596 | 100,122 | 10–13 | 76 177 (76) | 23 945 (24) | 2,659.3 | 348.1 | 264.9 | 83.3 | |
| 2028 | 766,847 | 101,312 | 10–13 | 76 825 (76) | 24 487 (24) | 2,663.7 | 347.5 | 263.5 | 84.0 | |
| 2029 | 778,099 | 106,264 | 10–14 | 77 173 (73) | 29 091 (27) | 2,668.0 | 359.7 | 261.2 | 98.5 | |
| 2030 | 789,350 | 107,079 | 10–14 | 78,001 (73) | 29 079 (27) | 2,672.4 | 357.8 | 260.6 | 97.2 | |
| Additional projectionsc | 2031 | 800,601 | 108,288 | 10–14 | 78,676 (73) | 29 612 (27) | 2,676.8 | 357.3 | 259.6 | 97.7 |
| 2032 | 811,853 | 108 728 | 10–13 | 79 485 (73) | 29 243 (27) | 2,681.2 | 354.3 | 259.0 | 95.3 | |
| 2033 | 823,104 | 109,871 | 10–13 | 80,293 (73) | 29,578 (27) | 2,685.6 | 353.7 | 258.5 | 95.2 | |
| 2034 | 834,356 | 109,254 | 9–13 | 81,004 (74) | 28,250 (26) | 2,690.0 | 347.6 | 257.7 | 89.9 | |
| 2035 | 845,607 | 110,058 | 9–13 | 81,692 (74) | 28,366 (26) | 2,694.4 | 346.1 | 256.9 | 89.2 | |
| 2036 | 856,858 | 109,024 | 9–13 | 82,419 (76) | 26,605 (24) | 2,698.8 | 338.9 | 256.2 | 82.7 | |
| 2037 | 868,110 | 109,804 | 9–13 | 82,983 (76) | 26,821 (24) | 2,703.2 | 337.6 | 255.1 | 82.5 | |
| 2038 | 879,361 | 110,740 | 9–13 | 83,796 (76) | 26,944 (24) | 2,707.6 | 336.7 | 254.8 | 81.9 | |
| 2039 | 890,613 | 111,910 | 9–13 | 84,529 (76) | 27,381 (24) | 2,711.9 | 336.6 | 254.3 | 82.4 | |
| 2040 | 901,864 | 113,206 | 9–13 | 85,683 (76) | 27,523 (24) | 2,716.3 | 336.9 | 255.0 | 81.9 | |
| 2041 | 913,115 | 114,695 | 9–13 | 86,850 (76) | 27,844 (24) | 2,720.7 | 337.8 | 255.8 | 82.0 | |
| 2042 | 924,367 | 116,140 | 9–13 | 88,016 (76) | 28,123 (24) | 2,725.1 | 338.6 | 256.6 | 82.0 | |
| 2043 | 935,618 | 117,922 | 9–13 | 89,384 (76) | 28,538 (24) | 2,729.5 | 340.3 | 257.9 | 82.4 | |
| 2044 | 946,870 | 119,465 | 9–13 | 90,560 (76) | 28,905 (24) | 2,733.9 | 341.3 | 258.7 | 82.6 | |
| 2045 | 958,121 | 121,059 | 9–13 | 91,815 (76) | 29,244 (24) | 2,738.3 | 342.5 | 259.8 | 82.7 | |
| 2046 | 969,372 | 122,498 | 9–13 | 92,933 (76) | 29,565 (24) | 2,742.7 | 343.2 | 260.4 | 82.8 | |
| 2047 | 980,624 | 123,480 | 9–13 | 93,700 (76) | 29,781 (24) | 2,747.1 | 342.6 | 260.0 | 82.6 | |
| 2048 | 991,875 | 125,058 | 9–13 | 95,018 (76) | 30,039 (24) | 2,751.4 | 343.7 | 261.2 | 82.6 | |
| 2049 | 1,003,127 | 126,578 | 9–13 | 96,152 (76) | 30,426 (24) | 2,755.8 | 344.6 | 261.8 | 82.8 | |
| 2050 | 1,014,378 | 128,600 | 9–13 | 97,713 (76) | 30,886 (24) | 2,760.2 | 346.9 | 263.6 | 83.3 | |
MBS = Medicare Benefits Schedule; NBCSP = National Bowel Cancer Screening Program
a ‘NBCSP % of MBS’ refers to the estimated percentage of MBS-recorded colonoscopies that would be generated by the NBCSP, based on those recorded as ‘private’ in the Australian Institute of Health and Welfare monitoring reports.
b NBCSP modelling for 2020 did not include any adjustments to screening participation or follow-up colonoscopy adherence attributable to the impact of the COVID-19 pandemic.
c Estimates for years after 2030 are subject to significant uncertainty and included as qualitative estimates.
It was estimated that there would be 94 809 NBCSP-related colonoscopies in 2019, which is 10–14% of the MBS-funded colonoscopies. Of these, 79% were index colonoscopies and 21% surveillance colonoscopies. In the absence of changes to NBCSP participation or iFOBT positivity rates, NBCSP-related colonoscopy use per capita would remain nearly constant from 2020 onwards. By 2030, the NBCSP was estimated to generate 107 079 colonoscopies, 10–14% of the projected MBS-funded colonoscopies. Of these, 73% were index colonoscopies and 27% surveillance colonoscopies. The proportions of colonoscopy by type are shown in Figure 2, for the periods 2006–2019 (during program rollout) and 2021–2030. Totals for each state and territory are shown in Supplementary Table 3, available from figshare.com/articles/dataset/Worthington_et_al_PHRP_2022_Supplementary_Tables_xlsx/21579570.The percentage of MBS-funded colonoscopies estimated to be attributable to the NBCSP ranged from 5% to 13% for the period 2006–2019, and from 9% to 14% for 2021–2030 (with the range representing the variation in the proportion of colonoscopies recorded by the MBS from 72.1 % to 100% as noted above).
Figure 2. Estimated proportion of MBS-funded colonoscopy demand in Australia by type, 2006–2019 and 2021–2030 (excluding 2020 as a significant outlier) (click to enlarge)
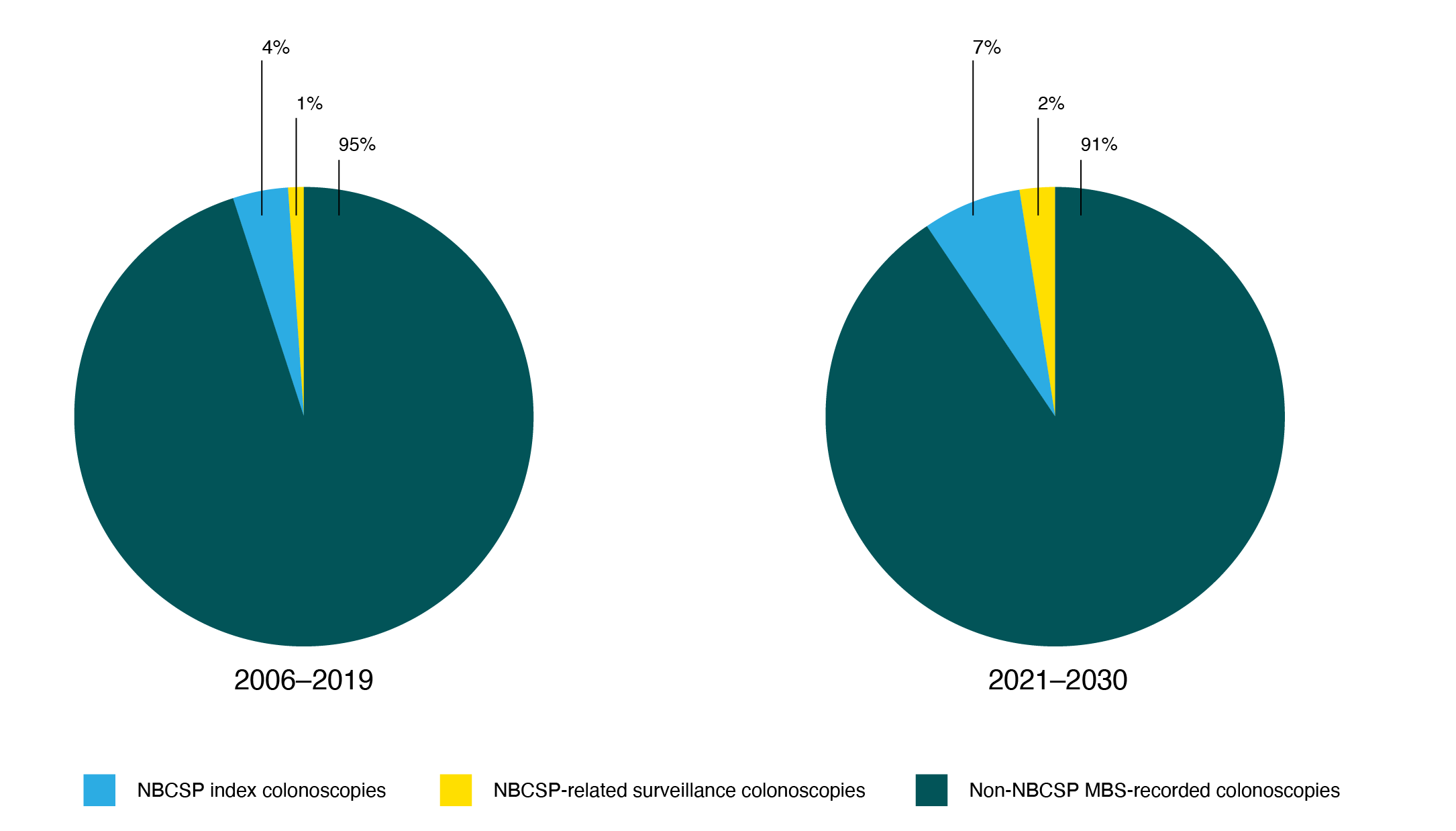
Note: For the purpose of this figure, 72.1% of NBCSP-generated colonoscopies were assumed to be recorded by the MBS (based on the proportion of NBCSP colonoscopies reported as occurring in the private system) – this is likely an underestimate. Estimates were used for total colonoscopy demand in 2021–2030.
Additional analysis
The results of the sensitivity analyses are presented in Supplementary Table 4 (available from: figshare.com/articles/dataset/Worthington_et_al_PHRP_2022_Supplementary_Tables_xlsx/21579570). If NBCSP participation increases to 56.6% from 2023, it is estimated that NBCSP-related colonoscopy use will be 22% higher than at current participation rates, with total annual colonoscopies increasing to 127 873 by 2030. If adherence to index colonoscopies was 80% instead of the currently modelled 66%, NBCSP-related colonoscopy use would be approximately 11% higher, with an annual total of 122 533 by 2030.
The results of the modelling using the pre-2019 surveillance colonoscopy guidelines for years after 2019 are shown in Supplementary Table 2 and Supplementary Figure 1 (available from figshare.com/articles/dataset/Worthington_et_al_PHRP_2022_Supplementary_Tables_xlsx/21579570), which demonstrate that the clinician use of the new guidelines may decrease annual colonoscopy use by 10%, without any changes to participation rates.
Discussion
This study quantifies colonoscopy use in Australia, including the impact of the NBCSP, and projects future rates. Our analysis shows that the NBCSP is estimated to contribute up to 10–14% of all MBS-funded colonoscopies. Colonoscopy use per capita has been increasing steadily but has started to slow; the trend over 2015–2019 from the linear projections show that colonoscopy use per capita has increased less than 0.2% per year (although this increase is not statistically significant). It is unclear what factors have driven the increases in colonoscopy demand, although much of the increase could be attributed to increases in underlying CRC in Australia22, alongside increases in CRC risk factors and health-seeking behaviours.
It is projected that the NBCSP will continue to contribute 10–14% of all MBS-funded colonoscopies to 2030 and beyond. Combined with previous studies, this analysis provides a clear argument that increasing participation in the program in line with government targets would increase overall colonoscopies modestly, while improving the effectiveness of the program overall.9 Even at the national target level of 56.6% screening participation in the invited cohort, the NBCSP still contributes only one-fifth of total colonoscopy use.
A core strength of this study is the use of Policy1-Bowel, a thorough microsimulation model capable of making long-term predictions. The NBCSP reached full rollout in 2019, meaning that cohorts are now experiencing full twice-yearly screening, so program-generated colonoscopy demand will grow before reaching an equilibrium. These nuances are captured in Policy1-Bowel and are reflected in our analysis.
The NBCSP is designed to provide screening to all average-risk individuals in Australia aged 50–74 years. Encouraging average-risk people to screen via the NBCSP would be a successful outcome, especially for average-risk individuals currently screening via colonoscopy; it is estimated that 8% of people use colonoscopy as first-line screening.23 If these individuals complete guideline-recommended iFOBT screening instead, the decrease in colonoscopy demand may balance potential increases from the NBCSP. Additionally, iFOBT-generated colonoscopies may be more likely to yield significant neoplastic findings such as adenomatous polyps or cancer. However, there are currently few data on this – ongoing monitoring of the NBCSP is essential.
By ensuring that colonoscopies are guideline recommended, colonoscopy demand and wait times could be reduced. Particularly at times of reduced supply, patients with a positive iFOBT test could be triaged to prioritise those at highest risk. This approach was taken by the Gastroenterological Society of Australia in 2020, when patients with positive iFOBTs were triaged as urgent24, and is used in some states and territories to triage patients for ‘direct access colonoscopy’.25
Prioritising program-based referrals over primary colonoscopy screening may also lead to improved equity in CRC outcomes. A review showed that remote areas and areas with a lower socioeconomic level have lower rates of colonoscopy use10 and higher rates of CRC deaths.7 Prioritising iFOBT-generated colonoscopies may improve accessibility of services, along with targeted campaigns to improve participation in these areas.26
There are several limitations to this study. Primarily, we do not have data on colonoscopies which were not funded and recorded by the MBS, as data on these colonoscopies are limited, incomplete, and dated.10 We were therefore not able to estimate the number of NBCSP-related colonoscopies which occur outside of MBS funding. We have included a range of estimates on the proportion of all colonoscopies which were not recorded by the MBS, and the qualitative conclusions are robust within this range. The migration of NBCSP data collection to the National Cancer Screening Register will hopefully improve the quality and consistency of NBCSP-related colonoscopy data collection.
We were not able to capture out-of-program screening, including colonoscopy screening and iFOBT screening led by GPs or available through other avenues. There are also limitations to how NBCSP-related colonoscopies are being reported, including underreporting and missing coding. As with all models, the modelling and extrapolation of MBS colonoscopies are limited by the assumptions made. These estimates are based on the assumption that there will not be any unexpected structural changes to screening in Australia. Estimates for years after 2030 are subject to a great deal of uncertainty; they have been included in this study with the caveat that they should be considered with caution.
As a result of the impact of the COVID-19 pandemic on the health system, MBS-related colonoscopy numbers for 2020 were an outlier and excluded from trend analysis. A previous study showed that monthly MBS-recorded colonoscopies dropped by more than 50% during 2020, but recovered to previously observed levels.27 However, the long-term impact of the pandemic is unclear – future studies will estimate these effects. Colonoscopy demand may increase from 2022 as individuals return to screening, and previously missed adenomas and other cancers are detected. A recent study found that this increase could be significant, but increasing the threshold for colonscopy referral following a positive iFOBT could help manage demand.
This work has not captured shifting colonoscopy use due to changing trends in CRC incidence in Australia. CRC incidence has increased in people under 50 years of age3, and it is unknown how CRC incidence will change in future. Any increase in CRC incidence would increase iFOBT positivity rates, and in turn colonoscopy use. Future modelling will incorporate these trends.
Conclusion
Ensuring that colonoscopy demand is manageable and performed per approved guidelines is critical to providing high-quality and high-value health services in Australia. Careful recording and coding of colonoscopy procedures and their indications in hospital records, including the referral source (NBCSP or other), date and result, are critical in assessing the true demand for colonoscopy, as well as highlighting areas for improvement to ensure that colonoscopies are providing the highest possible value. This study shows that colonoscopy use will increase over time, based on past trends, but the NBCSP is unlikely to contribute to excess demand. Combined with previous studies on the health and cost benefits of the NBCSP, supporting continued and increased use of the iFOBT could contribute to relieving concerns about colonoscopy demand in Australia.
Acknowledgements
PG reports his former employer, Cancer Council Australia, received Australian Government funding in 2014–17 to develop national clinical practice guidelines for CRC, which included guidelines on colonoscopy.
KC’s research is funded by the National Health and Medical Research Council (NHMRC) of Australia (Fellowship APP1194679, Centre for Research Excellence in Cervical Cancer Control 1135172). JBL’s research is funded by an NHMRC Investigator grant (APP1194784). EF receives NHMRC grant funding to investigate improving participation in the NBCSP (APP2014964).
The Daffodil Centre through Cancer Council Australia, which employs authors JW, EH, JBL, PG, KC and EF, has received Australian Government funding in to update chapters of the national clinical practice guidelines for CRC chapters on population screening (covering the NBCSP) and risk and screening based on family history. This project is ongoing.
Peer review and provenance
Externally peer reviewed, not commissioned.
Copyright:

© 2022 Worthington et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Australian Institute of Health and Welfare. Cancer data in Australia; 2020 [cited 2022 Jul 7]. Canberra: AIHW; 2020. Available from: www.aihw.gov.au/reports/cancer/cancer-data-in-australia
- 2. Goldsbury DE, Feletto E, Weber MF, Haywood P, Pearce A, Lew J-B, et al. Health system costs and days in hospital for colorectal cancer patients in New South Wales, Australia. PloS one. 2021;16(11):e0260088. CrossRef | PubMed
- 3. Feletto E, Yu XQ, Lew J-B, St John DJB, Jenkins MA, Macrae FA, et al. Trends in Colon and rectal cancer incidence in Australia from 1982 to 2014: analysis of data on over 375,000 cases. Cancer Epidemiol Biomarkers Prev. 2019;28(1):83–90. CrossRef | PubMed
- 4. Cienfuegos J-A, Baixauli J, Martínez-Ortega P, Valentí V, Martínez-Regueira F, Martí-Cruchaga P, et al. Screening-detected colorectal cancers show better long-term survival compared with stage-matched symptomatic cancers. Revista Española de Enfermedades Digestivas. 2018;110(11):684–90. CrossRef | PubMed
- 5. Lew JB, St John DJB, Macrae FA, Emery JD, Ee HC, Jenkins MA, et al. Evaluation of the benefits, harms and cost-effectiveness of potential alternatives to iFOBT testing for colorectal cancer screening in Australia. Int J Cancer. 2018;143(2):269–82. CrossRef | PubMed
- 6. Cancer Council Australia Colorectal Cancer Guidelines Working Party. Clinical practice guidelines for the prevention, early detection and management of colorectal cancer 2017. Sydney: Cancer Council Australia; 2017 [cited 2022 Jul 7]. Available from: www.cancer.org.au/health-professionals/clinical-practice-guidelines/colorectal-cancer
- 7. Australian Institute of Health Welfare. National Bowel Cancer Screening Program: monitoring report 2020. Canberra: AIHW; 2020 [cited 2022 Jul 7]. Available from: www.aihw.gov.au/reports/cancer-screening/national-bowel-cancer-screening-monitoring-2020/summary
- 8. Clarke L, Pockney P, Gillies D, Foster R, Gani J. Time to colonoscopy for patients accessing the direct access colonoscopy service compared to the normal service in Newcastle, Australia. Intern Med J. 2019;49(9):1132–7. CrossRef | PubMed
- 9. Lew JB, St John DJB, Xu XM, Greuter MJE, Caruana M, Cenin DR, et al. Long-term evaluation of benefits, harms, and cost-effectiveness of the National Bowel Cancer Screening Program in Australia: a modelling study. Lancet Public Health. 2017;2(7):e331–e40. CrossRef | PubMed
- 10. Australian Commission on Safety and Quality in Health Care. Australian Atlas of Healthcare Variation 2015: Chapter 2.1 Fibre optic colonoscopy. Sydney: ACSQHC; 2015 [cited 2022 Jul 7]. Available from: www.safetyandquality.gov.au/publications-and-resources/resource-library/australian-atlas-healthcare-variation-2015-chapter-21-fibre-optic-colonoscopy
- 11. Australian Government, Services Australia. Medicare item reports. Canberra: Services Australia; 2021 [cited 2022 Jul 7]. Available from: https://medicarestatistics.humanservices.gov.au/
- 12. Zorzi M, Hassan C, Capodaglio G, Baracco M, Antonelli G, Bovo E, et al. Colonoscopy later than 270 days in a fecal immunochemical test-based population screening program is associated with higher prevalence of colorectal cancer. Endoscopy. 2020;52(10):871–6. CrossRef | PubMed
- 13. Lin JS, Perdue LA, Henrikson NB, Bean SI, Blasi PR. Screening for colorectal cancer: An evidence update for the US Preventive Services Task Force. JAMA. 2021;325(19):1965–77. 34003218 CrossRef | PubMed
- 14. Feletto E, Grogan P, Nickson C, Smith M, Canfell K. How has COVID-19 impacted cancer screening? Adaptation of services and the future outlook in Australia. Public Health Res Pract. 2020;30(4):e3042026. CrossRef | PubMed
- 15. Australian Institute of Health and Welfare. Cancer screening programs: quarterly data Canberra; AIHW; 2021 [cited 2022 Jul 7]. Available from: www.aihw.gov.au/reports/cancer-screening/national-cancer-screening-programs-participation
- 16. Australian Bureau of Statistics. 3101.0 – Australian demographic statistics, Dec 2019. Canberra: ABS; 2020 [cited 2022 Jul 7]. Available from: www.abs.gov.au/ausstats/[email protected]/mf/3101.0
- 17. Australian Bureau of Statistics. Population Projections, Australia, 2017 (base) to 21012018. Canberra: ABS; 2021 [Cited 2022 Jul 7]. Available from: www.abs.gov.au/statistics/people/population/population-projections-australia/latest-release
- 18. Cancer Council Australia. Colonoscopy Surveillance Working Party. Clinical practice guidelines for surveillance colonoscopy – in adenoma follow-up; following curative resection of colorectal cancer; and for cancer surveillance in inflammatory bowel disease. Sydney: Cancer Council Australia; 2011 [cited 2022 Jul 7]. Available from: www.colonoscopyclinic.com.au/wp-content/uploads/2017/11/cpgcs.pdf
- 19. Cancer Council Australia. Surveillance Colonoscopy Guidelines Working Party. Clinical practice guidelines for surveillance colonoscopy. Sydney: Cancer Council Australia; 2019 [cited 2022 Jul 7]. Available from: www.cancer.org.au/health-professionals/clinical-practice-guidelines/colorectal-cancer
- 20. Commonwealth of Australia. Portfolio budget statements 2020–21 Budget Related Paper No. 1.7. Health Portfolio. Canberra: Department of Health; 2020 [cited 2022 Jul 7]. Available from: www.health.gov.au/sites/default/files/documents/2020/10/budget-2020-21-health-portfolio-budget-statements.pdf
- 21. Symonds EL, Simpson K, Coats M, Chaplin A, Saxty K, Sandford J, et al. A nurse‐led model at public academic hospitals maintains high adherence to colorectal cancer surveillance guidelines. Med J Aust. 2018;208(11):492–6. CrossRef | PubMed
- 22. Luo Q, Lew J-B, Steinberg J, Worthington J, Yu XQ, Caruana M, et al. Trends in colon and rectal cancer mortality in Australia from 1972 to 2015 and associated projections to 2040. Sci Rep. 2022;12(1):3994. CrossRef | PubMed
- 23. Emery JD, Pirotta M, Macrae F, Walker JG, Qama A, Boussioutas A, et al. 'Why don't I need a colonoscopy?': A novel approach to communicating risks and benefits of colorectal cancer screening. Aust J Gen Pract. 2018;47(6):343–9. CrossRef | PubMed
- 24. Gastroenterological Society of Australia (GESA). Guide for triage of endoscopic procedures during the COVID-19 pandemic. 2020 [cited 2022 Jul 7]. Available from: www.gesa.org.au/public/13/files/Education%20%26%20Resources/COVID-19/Triage_Guide_Endoscopic_Procedure_26032020.pdf
- 25. NSW Agency for Clinical Innovation. NSW colonoscopy categorisation. Sydney: ACI; Aug 2020 [cited 2022 Jul 7]. Available from: https://aci.health.nsw.gov.au/resources/gastroenterology/nsw-colonoscopy-categorisation/nsw-colonoscopy-categorisation
- 26. Worthington J, Feletto E, Lew J, Broun K, Durkin S, Wakefield M, et al. Evaluating health benefits and cost-effectiveness of a mass-media campaign for improving participation in the National Bowel Cancer Screening Program in Australia. Public Health. 2020;179:90–9. CrossRef | PubMed
- 27. Cancer Australia. National and jurisdictional data on the impact of COVID-19 on medical services and procedures in Australia: breast, colorectal, lung, prostate and skin cancers. Sydney; Australian Government; 2020 [cited 2022 Jul 7]. Available from: www.canceraustralia.gov.au/National_and_jurisdictional_data_on_the_impact_of_COVID-19_on_medical_services_and_procedures