Abstract
Introduction: The coronavirus disease 2019 (COVID-19) pandemic has exacerbated financial strain among populations worldwide. This is concerning, given the link between financial strain and health. There is little evidence to guide action in this area, particularly from a public health perspective. To address this gap, we examined initiatives to address financial wellbeing and financial strain in high-income contexts.
Methods: We used rapid review methodology and applied an equity-focused lens in our analysis. We searched six databases (MEDLINE, PsycINFO, Web of Science, ProQuest, Informit, and Google Advanced) for peer-reviewed, academic and practice-based literature evaluating initiatives to address financial strain and wellbeing in high-income contexts published between 2015–2020. We conducted a relevancy and quality appraisal of included academic sources. We used EPPI-reviewer software to extract equity-related, descriptive data, and author-reported outcomes.
Results: We conducted primary screening on a total of 4779 titles/abstracts (academic n = 4385, practice-based n = 394); of these, we reviewed 182 full text articles (academic n = 87, practice-based n = 95) to assess their relevancy and fit with our research question. A total of 107 sources were excluded based on our selection criteria and relevance to the research question (Figure 1), leaving 75 sources that were extracted for this review (academic n = 39, practice-based n = 36). These sources focused on initiatives predominantly based in Australia, the US, and Canada, with a smaller number from the UK and Europe. Most sources primarily targeted financial literacy and personal/family finances, followed by employment, housing, and education.
Conclusions: We found that holistic initiatives (i.e., complex, wrap-around) that ensured people’s basic needs were met (for example, before building financial skills) were aligned with positive and equitable financial wellbeing and financial strain outcomes, as reported in the reviewed studies. We noted significant gaps in the literature related to equity, such as the impact of initiatives on socially excluded populations (e.g., Indigenous peoples, racialised peoples, and rural dwellers). More research using a public health lens is required to guide equitable and sustainable action in this area.
Full text
Introduction
Financial circumstances have a direct impact on health outcomes in adults and children.1-3 Financial strain, more specifically, is associated with poor physical and mental health1-3 and work absenteeism.4 Financial strain describes the stress of worrying about an imbalance between income and expenditures.5 In contrast, financial wellbeing indicates an absence of financial strain where a person has financial security now and in the foreseeable future.6 Financial strain is conceptually similar to financial distress, stress, economic strain, financial health, and financial wellbeing. It differs, however, from poverty, indebtedness, employment status, and income, which categorise people’s financial status based on quantifiable measures of their financial circumstances.5 Financial strain has an impact on health independent of these measures.7,8 It can lead to the deterioration of self-esteem and social relationships.5,9
The link between financial strain and health is an emerging area of research and practice in public health.5,10,11 As a result, there is a lack of evidence focused on initiatives addressing the structural and systemic factors underpinning financial strain.12 Instead, individual-level behavioural interventions predominate.12 The coronavirus 2019 disease (COVID-19) pandemic highlighted the way in which structural factors (e.g. pandemic policy-making) can determine health, social, and economic outcomes..13 Governments and organisations acted – to varying degrees – to stem the growing inequities and support people’s health and overall wellbeing, economic and otherwise, during the pandemic.14 Although many jurisdictions have now shifted to a ‘living with COVID’ period, there remains an urgent need for initiatives to address ongoing financial strain, which disproportionately impacts systemically excluded groups.15
This review was part of a larger project that created a practice-oriented framework16 and a guidebook of strategies and indicators17 to promote financial wellbeing, informed by a public health perspective.16 To ground the development of the framework and guidebook to promote financial wellbeing, we conducted a rapid review to identify and describe initiatives targeting personal and household financial strain and wellbeing in high income economies.18 We applied an equity lens19 to understand factors related to equitable impact and identify literature gaps.
Methods
We have published the methods for the broader project elsewhere.16,17 For this study, we followed rapid review methods20 and applied an equity lens21 to conduct an inductive narrative synthesis22 of the literature. We took a systematic approach to the search strategy using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines23 and conducted separate searches for peer-reviewed and practice-based literature. We conceptualised financial strain as a present, subjective aspect of financial wellbeing, where the presence of financial strain indicated a lack of financial wellbeing.6 The term ‘initiative’ is used to describe different actions taken to promote financial wellbeing, and is herein used to describe such actions. However, various terms were used in our search strategy to identify relevant papers (See Supplementary Tables 1 and 2, available from: doi.org/10.6084/m9.figshare.23120978).
Peer-reviewed literature search strategy
We conducted a search of the following databases for studies published between 2015 and August 2020: MEDLINE, PsycINFO, and Web of Science (Social Science Citation Index) using a two-concept search: i) financial strain and/or financial well-being; AND ii) initiative. We added the following limits to the search: English-language and full-text available. A research librarian designed and ran the searches on 13 August 2020. Details and results are provided in Supplementary Table 1 (available from doi.org/10.6084/m9.figshare.23120978).
Practice-based literature search strategy
We conducted a search for practice-based sources using two databases (ProQuest and Informit) and filtered the search results by source type (e.g., reports, other articles). We adapted the search terms and limitations used in the peer-reviewed strategy to create a set of search strings (See Supplementary Table 2, available from doi.org/10.6084/m9.figshare.23120978) that we input into Google Advanced search. We executed the searches using the ‘private’ browser setting and reviewed the first 200 hits. The search was limited to sources published in or after 2015. We took an iterative approach to the search and continued until new searches were not retrieving many new, potentially relevant sources.
Inclusion and exclusion criteria
We applied the following inclusion criteria to all sources: i) evaluated an initiative targeting financial strain or financial wellbeing; ii) high-income context18; iii) published after 2015; and iv) English. We excluded sources if i) they were reviews, study protocols, commentaries, editorials, books, or theses; ii) they did not describe the results of an initiative, including empirical research on a process or outcome evaluation of an initiative using qualitative, quantitative, or mixed-methods, or had a companion source with information about an evaluated initiative; iii) the primary focus of the initiative was not financial strain and/or financial wellbeing as defined for this study; or iv) they did not have the potential to contribute meaningfully to answering the research question.
Study selection
We uploaded the retrieved peer-reviewed sources to EPPI-Reviewer software (Version 4) for title/abstract and full-text screening. Using the inclusion and exclusion criteria, two independent reviewers conducted title and abstract screening, any discrepancies were discussed, and a consensus was reached. We followed the same process for full-text article screening. Three reviewers piloted the screening process to assess reliability before we proceeded. We discussed discrepancies among at least two independent reviewers to reach a consensus. To ensure the diversity of the sources and alignment with the research purpose, we prioritised sources for final inclusion that reported on initiatives in: Canada, Australia, and non-US developed economies; in rural locations; targeting Indigenous peoples, Native Americans, and/or Aboriginal peoples; and, representing a diversity of settings, levels, types, and targets.
For the practice-based sources, a single reviewer conducted the primary screening against the inclusion and exclusion criteria based on the title and/or link and text available on the search engine home site. For this reason, we undertook the search and primary screening simultaneously for practice-based sources. We reviewed the first 200 hits retrieved through each search and recorded full-text sources in an Excel sheet. A single reviewer screened all full texts of practice-based sources, and a 10% sample was reviewed by an additional reviewer.
Quality & relevance appraisal
We used the Mixed Methods Appraisal Tool (MMAT)24 to describe the quality of peer-reviewed sources that reported on empirical research. None of the peer-reviewed sources were excluded based on the response to the MMAT screening questions.
Data extraction & synthesis
We created a detailed data extraction tool using EPPI-Reviewer to capture the initiative level, type, design, and context (e.g. setting, environment). We extracted data related to health equity using the principles defined by the Public Health Agency of Canada tool to develop equity-sensitive initiatives.19. We included: equity objectives, social determinants of health (SDoH), and equity target (i.e. whether the initiative was universal, targeted, or proportionate in its delivery)19, and if the targeted population included systemically excluded groups such as racialised and/or Indigenous peoples, women, and recently arrived immigrants The ‘effectiveness’ of initiatives was not explicitly analysed. Rather, where outcomes of initiatives were reported in studies, these were captured and included in the synthesis. Results of an in-depth critical realist analysis of included papers are reported elsewhere.25
Results
A total of 4385 peer-reviewed sources were included in primary screening, with title screening n= 3516) and abstract screening (n = 261) completed in separate steps. For practice-based sources only the first 200 hits of each search string were included (see Supplementary Table 2 for practice-based search strategy, available from doi.org/10.6084/m9.figshare.23120978), leaving a total of 394 practice-based sources that were included in primary screening, whereby titles and abstracts were screened in the same step. After primary screening was complete a total of 182 sources remained which were included in the full text review (peer-reviewed n = 87; practice-based n = 95). Once full texts were reviewed against our selection criteria, and relevance to our research question, a further 107 sources were excluded, leaving 75 sources (peer-reviewed n = 39, practice-based n = 36) in the final extraction. We outline the process and reasons for exclusion in Figure 1. A brief description and summary of characteristics for all included sources are provided in Supplementary Tables 3 (academic sources) and 4 (practice-based sources, available from doi.org/10.6084/m9.figshare.23120978). References for all papers included in the review process are listed in Supplementary Table 5 (available from doi.org/10.6084/m9.figshare.23120978). Most sources used a quantitative approach, including non-randomised (n = 23), randomised controlled trial (n= 4), descriptive (n = 4), and natural experiment (n = 1) designs; followed by mixed-methods (n = 27) and qualitative (n = 16) designs. The study design was unclear for four practice-based sources due to the lack of methods descriptions.S2,S60,S63,S67
Figure 1. PRISMA flow chart of included sources (click figure to enlarge)

PB = practice-based sources; PR = peer-reviewed sources
Most sources were from Australia (n= 25), the US (n = 24), and Canada (n = 10), followed by the UK (n = 6) and the EU-27 (i.e., all European Union countries together) (n = 2). The remaining sources (n = 10) were located in the following countries: Switzerland, Denmark, Spain, Austria, Sweden and New Zealand. Where identified, initiatives were largely undertaken in urban (n = 34) compared to rural (n = 11) environments. We classified the initiatives by setting, which included society (i.e. policy or government) (n = 33), community (e.g., local, neighbourhood) (n = 27), school (n = 3), healthcare (n = 3), and workplace (n = 1). The setting for six initiatives was unclear, and two took place in multiple settings.
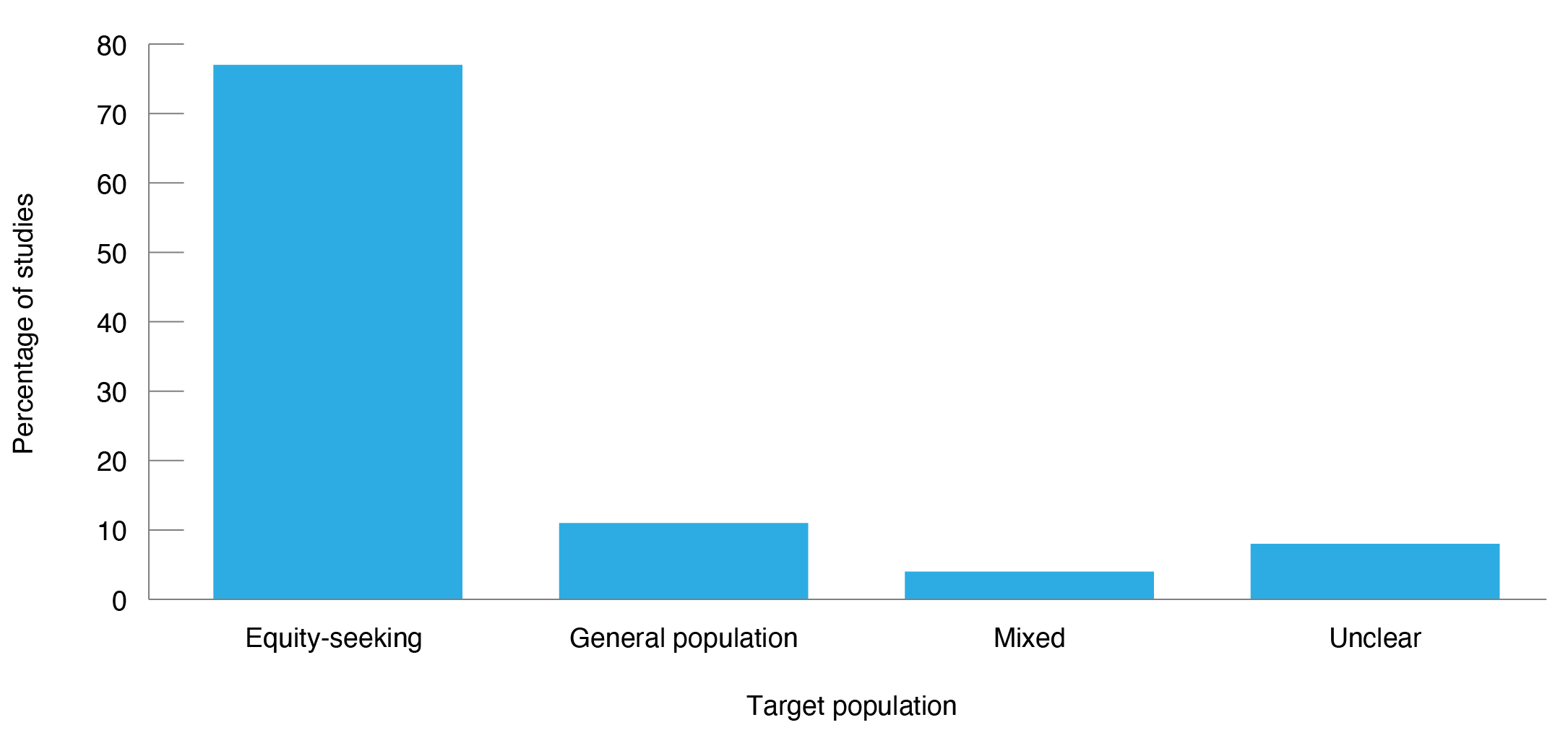
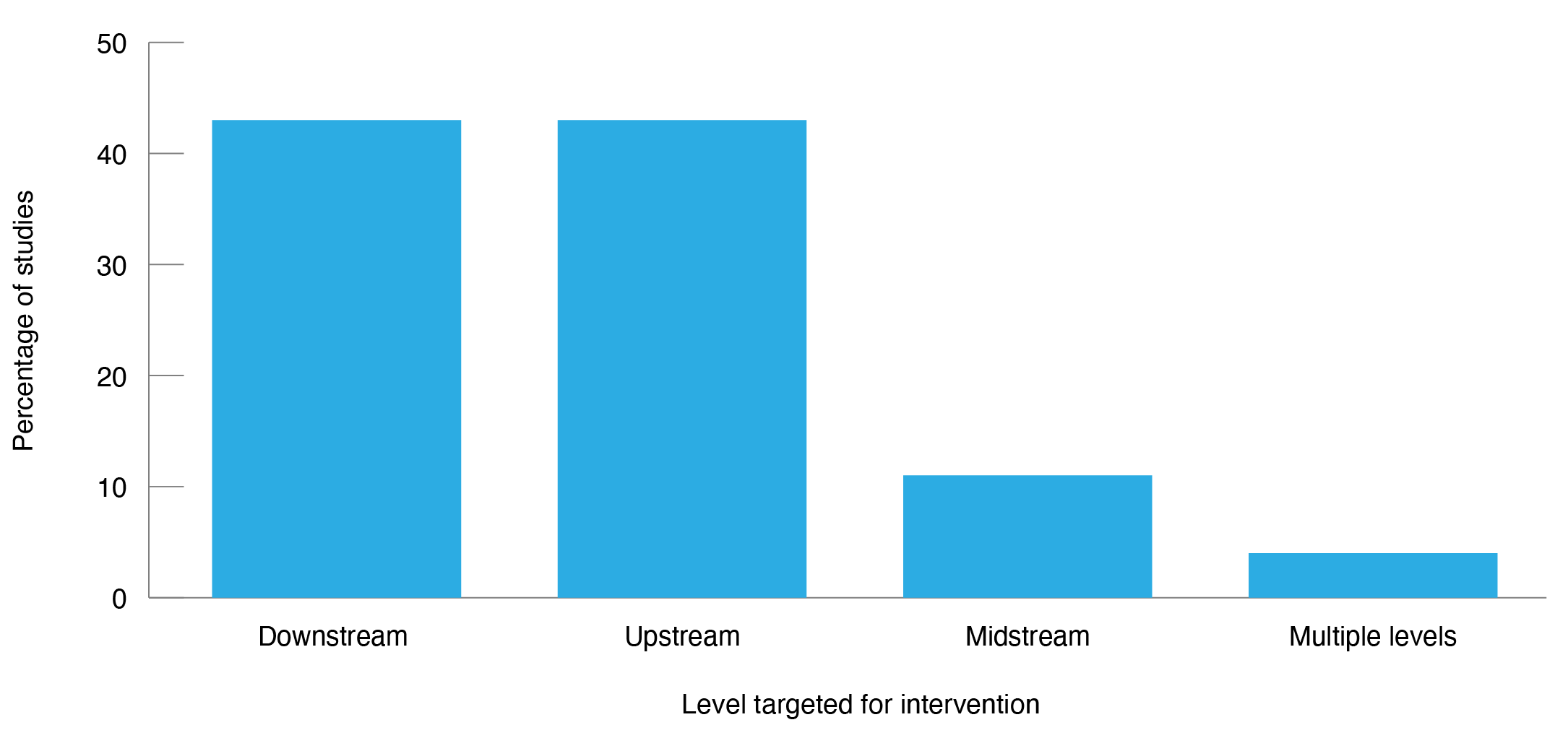
Figure 2 shows the characteristics of source initiatives and their target populations in relation to the equity principles previously defined.19,21 In many sources, the initiatives targeted multiple areas or foci. In terms of equity orientation19, we found that the source initiatives were mainly targeted (i.e. focused on distinct populations) (n = 27), followed by universal (i.e. focused on everyone) (n = 11), and studies combining universal and targeted initiatives (n = 10). Initiatives were largely balanced between downstream (i.e., focused on behaviour change) (n = 32) and upstream (i.e., focused on changing socioeconomic environments) (n = 32 actions; with the majority (n = 56) focused on systemically excluded populations. Systemically excluded populations broadly included people with low or no income, including people facing unemployment (n = 29), and more specifically: people experiencing or at risk of homelessness (n = 9); Indigenous peoples (n = 5); older people (n = 5); single mothers (n = 3); people experiencing disability (n = 3); caregivers (n = 3); refugees and immigrants (documented and undocumented) (n = 3); and children and youth in or leaving out-of-home care (i.e., transitioning out of care) (n= 2).
Figure 2. Characteristics of source interventions and target groups for interventions
2a) Target population for included studies (N = 75) (click figure to enlarge)
2b) Target area for included studies (N = 156a) (click figure to enlarge)
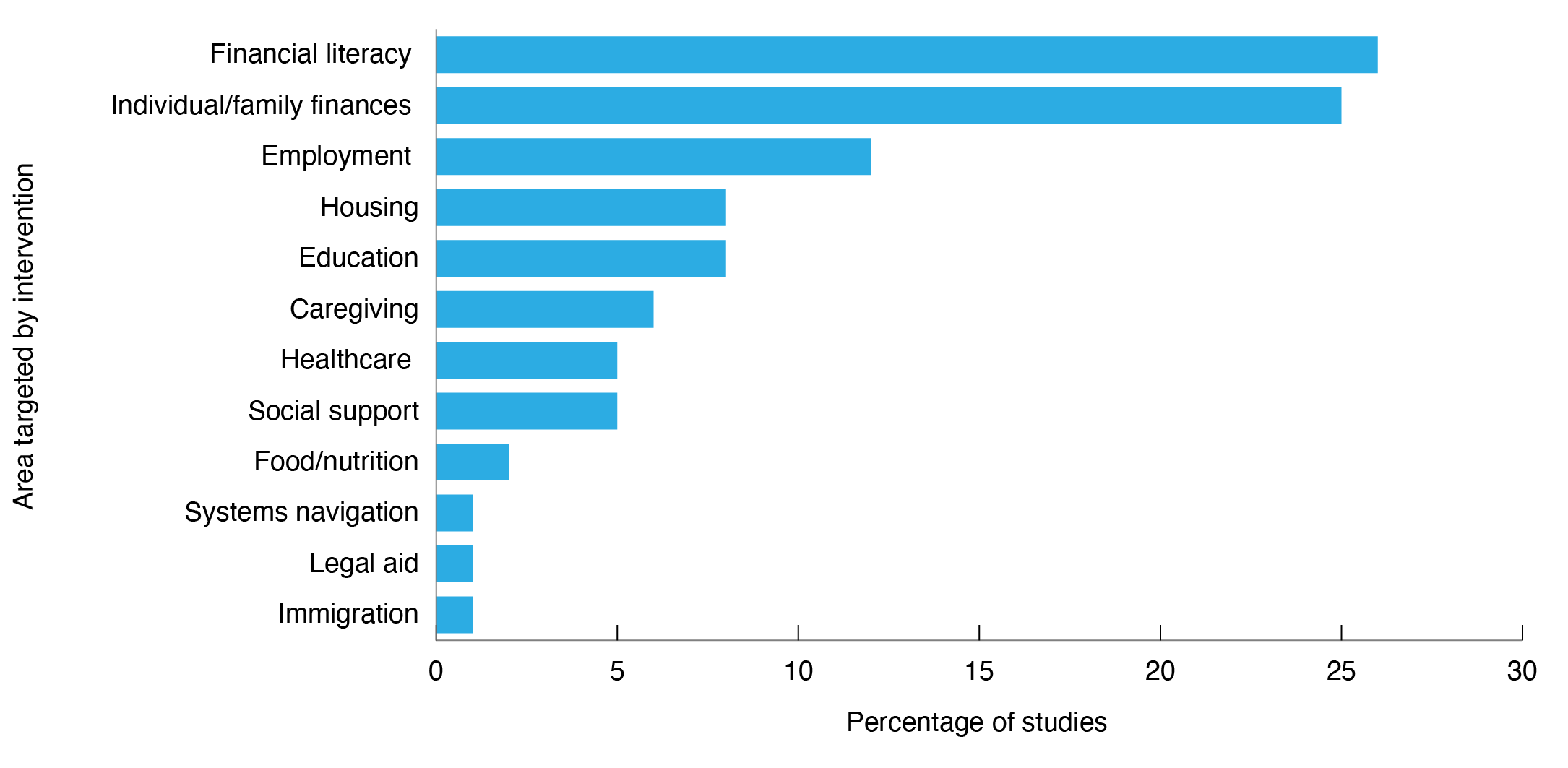
a Some of the 75 included studies targeted multiple areas and are represented in more than one category.
2c) Intervention setting for included studies (N = 75) (click figure to enlarge)
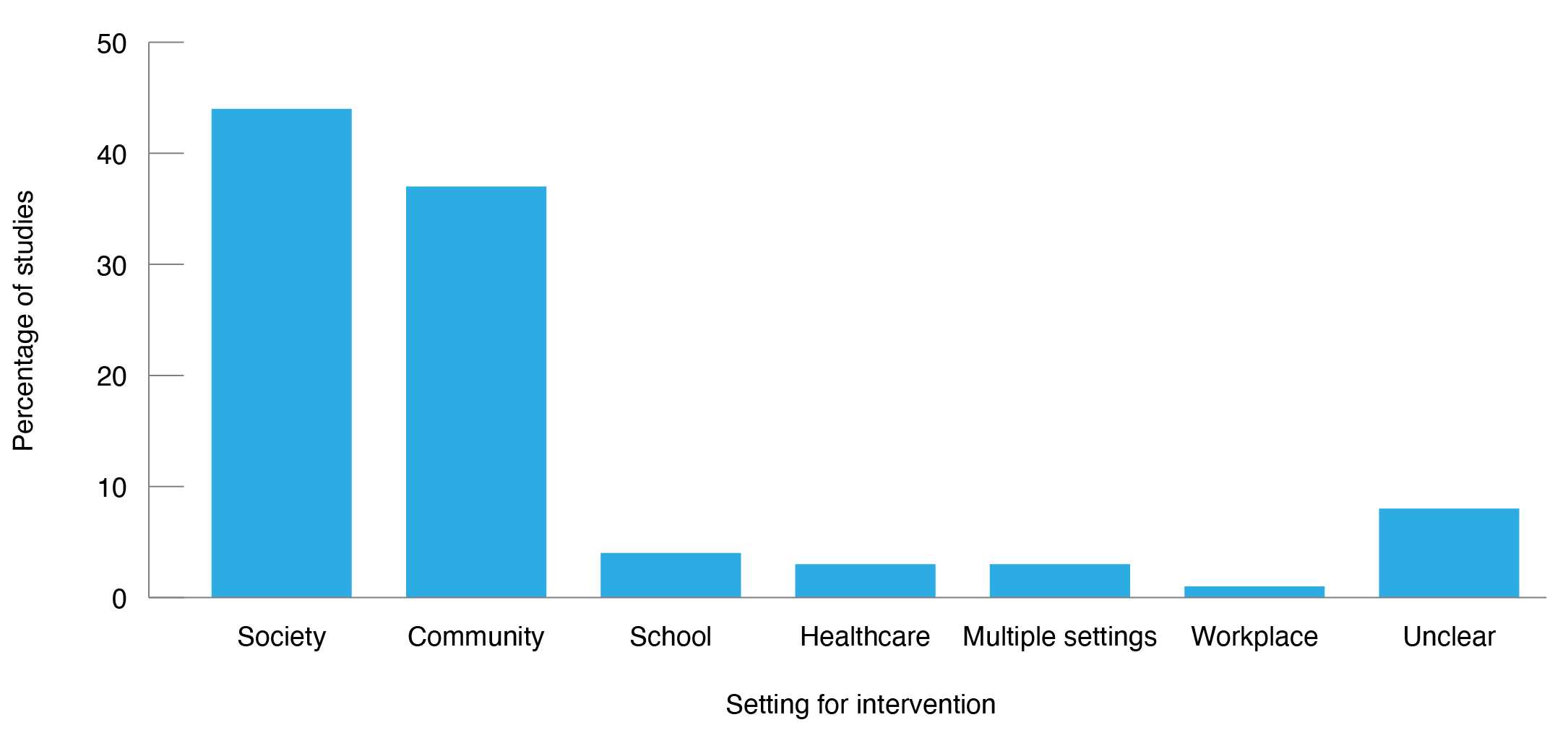
Figure 2c) Intervention setting for included studies (N = 75)
2d) Intervention level for included studies (N = 75) (click figure to enlarge)
Intervention impacts on financial wellbeing
Financial literacy initiatives (n = 41) were the most prominent target area (Figure 2), and these targeted individual behaviour change. The reported effectiveness of financial behaviour change initiatives was limited, particularly where they were not paired with wrap-around services addressing structural inequity related to, for example, housing, education and unemployment. Key areas that determined the reported effectiveness of financial literacy initiatives included awareness of and access to financial knowledge, as well as advice on how to manage credit and debtS4,S7,S14,S26,S60,S62,S72; resilience and confidence buildingS4,S7,S11,S12,S14,S74, self-identified need for financial assistanceS12,S14,S26,S62, and, self-perception of financial progress, future, and goals.S4,S7,S12,S15,S16,S60,S62,S72 In the US, a person’s debt/credit score also impacted financial decision making, which had a subsequent consequence on the reported effectiveness of individualised programs.S16,S60,S68,S69
Initiatives targeting personal/family finances (n = 39) were also prominent and included cash benefits, welfare payments, and income management. Strong social welfare benefits, including universal and targeted types of social equity policies that covered or extended beyond basic needs and had minimal contingencies and barriers to access, positively impacted financial wellbeing. This was particularly so among systemically excluded groupsS24, non-citizen and racialised immigrantsS75, and older women.S37 Conditions that constrained the accessibility and reported the effectiveness of social welfare benefits included: the rising pension ageS2; work for welfare programsS5,S21,S23,S24,S30; mandatory attendance at job seeking meetings and complex administrative requirementsS6,S10,S25,S59; citizenship and immigration status-related restrictionsS75; tax-exemption-based benefits prioritising two-parent families.S13 Other factors reported to have impacted the effectiveness of these benefits were: breadwinner-based family and labour policies that incentivised traditional gender roles and women’s dependence (e.g., household taxation, preferential training/employment for men)S37; and eligibility requirements that did not consider complex social locations including Indigenous peoplesS5,S59; asylum seekersS1,S57; people who experience homelessnessS57; undocumented immigrantsS75; caregiversS27,S20; and mothersS32,S37,S21, including single mothers.S13,S25
All but one of the initiativesS43 that targeted employment (n = 18) incorporated other components. In most cases, employment was paired with initiatives to address personal/family finances (including the provision of social welfare).S4,S5,S10,S18,S21,S22,S43,S45,S46,S54,S66,S73 However, some initiatives providing financial literacyS9,S21,S46,S33,S4,S10,S11,S35,S53, education, social supportS21,S22,S10,S11,S63, housingS22,S4,S11,S10,S63, healthcareS4,S18,S22, and caregivingS4,S45, also included an employment component. In the US, providing standalone financial coaching services among unemployed people was reported ineffective unless paired with employment support.S68 Coupling social welfare benefits with employment conditions and outcomes created barriers to promoting financial wellbeing. In the US, a conditional cash transfer initiative with strict employment conditions that occurred during the 2007–2009 recessionS18 and a homeownership program (Housing Plus)S51 created barriers leading to participant disengagement and dropout. Two examples from Australia that coupled social welfare (cash benefits) with employment outcomes among remote Indigenous peoplesS5, and single mothersS25, increased impoverishment, stress, and anxiety among recipients.
We noted that housing (n = 13) and education (n = 12) initiatives were less prominent than employment and individual/household finance initiatives (Figure 2), despite being associated with improvements in financial wellbeing, particularly when part of a holistic or wrap-around approach. Housing initiatives included assistance in securing housing for homeless peopleS56, interest-free loansS33 or bursary paymentsS11,S63to cover rent and housing expenses, subsidised housingS10,S42,S22, shared homeownershipS65, and a US-based wrap-around home ownership support program known as Housing PlusS51 (i.e., low mortgage rates, escrow savings, matched down payment savings, education, financial inclusion).S51 In general, longer-term housing initiatives were more impactful than short-term programs to promote housing security and financial wellbeing.S10,S22,S42Initiatives that improved access to education also positively impacted financial wellbeing. These included: a bursary program for young Australian caregivers that allowed participants to study and work towards sustainable employmentS27; a wrap-around service linking people leaving out-of-home care with free community college coursesS63; and an early life education initiative that promoted cumulative socioeconomic advantage.S50 A financial coaching initiative that also provided literacy and numeracy training contributed small increases (12%) in job placement rates, hourly wages, and net monthly income.S35
A limited number of sources we reviewed included a component supporting access to healthcare (n = 8). In the US, a study reporting extended access to Medicaid via the Patient Protection and Affordable Care Act (known as.”Obamacare”) had a beneficial impact on healthcare-related financial strain and economic uncertainty of people at up to 199% above the Federal poverty line, demonstrating its positive equity impact.S41 A US policy providing comprehensive caregiver support to the partners of injured veterans, including access to physical and mental healthcare, positively impacted financial strain.S55 However, strict eligibility criteria hampered participation in the program. Two Australian initiatives that included a component facilitating access to healthcare for at-risk youthS10 and recent immigrants and refugeesS57 reported positive impacts on physical and financial wellbeing.
Identified literature included initiatives targeting social support (e.g., connecting people with social services) (n = 8) as part of multifaceted initiatives.S19,S21,S48,S10,S11,S56,S63 All but twoS19,S21of these focused on housing initiatives to improve financial wellbeingS22,S48,S10,S11,S56,S63among people with little to no incomeS21, those experiencing or at risk of homelessnessS19,S22,S11,S56, and/or involved people living in out-of-home care.S10,S63
Discussion
This rapid review aimed to identify and describe peer-reviewed and practice-based literature that evaluated community-led and government initiatives targeting financial wellbeing and financial strain in high-income economies. We also assessed the initiatives through an equity lens. The review showed that initiatives seeking to improve financial wellbeing were largely focused on financial capability – including financial skills, knowledge, and attitudes – and targeted individual behaviour change. This aligns with previous research conducted in the area.12,26 However, evidence from the included sources highlighted the limitations of these initiatives when not coupled with other components addressing structural inequity with regard to having a long-term positive impact on financial wellbeing or financial strain. A systematic review27 examining the equity impact of various interventions reported that ‘downstream’ behaviour change initiatives did not reduce health and social inequities and might even exacerbate them. Despite evidence demonstrating that complex system-focused solutions can potentially reduce inequities more sustainably than individual behavioural initiatives28, the latter remains socially and politically attractive because it places the responsibility for change on the individual rather than the government, systems or society. The review showed that initiatives that applied holistic and flexible approaches, including structural approaches – such as addressing housing factors – were reported to be effective in enhancing the accessibility of services and benefits and providing longer-term pathways toward sustained financial wellbeing. Holistic initiatives often included wrap-around support and/or bundled multiple services into one program (e.g. food, clothing)S10, ‘living skills’ developmentS4,S11, or education pathways.S22
In this review, we identified several equity-relevant19,21gaps in the literature. Specifically, evaluations of initiatives targeting financial wellbeing rarely assessed outcomes related to equity-relevant social locations and/or SDoH, including age, ability, and race. This is unsurprising, given that many countries do not collect robust data to enable disaggregation by disability29 or race/ethnicity.30 Issues surrounding data disaggregation and equity became markedly apparent at the onset of the COVID-19 pandemic, where a lack of visibility and representation heightened risk and impacted health and economic response planning.30,31 Many sources assessed outcomes related to education level and/or sex. To ensure equitable approaches to policy and planning now and in the future, we suggest that data on outcomes and impacts of interventions be disaggregated by age, ability, and race, in addition to gender identities and education.
Overall, we found that initiatives accounting for diverse cultural values were received positivelyS26,S71,S66, and were in some instances reported to be effective in reducing short-term financial strain.S71 Yet few initiatives were tailored to racially minoritised populations – specifically Black, Hispanic, or Indigenous peoplesS5,S18,S32– despite the over-representation of these groups among people experiencing financial strain. In addition, COVID-19 has exacerbated health32 and economic33 risks among these groups. We found that initiatives targeting financial behaviour change had a relative over-representation of participants who were racialised primarily Black and Hispanic, with these groups comprising up to 70% of initiative participantsS16,S68,S39,S61,S69,S70, yet they failed to tailor initiatives to the complex sociocultural needs of these groups. Moreover, there were no Canadian initiatives identified that were created for Indigenous peoples, even though approximately one-quarter of urban Indigenous peoples in Canada live in poverty.34
Our review identified a lack of community-led and participatory-based initiatives. Previous reviews in health and policy have reported that collaboration and participatory approaches support cultural appropriateness, enhance recruitment, build capacity, minimise health inequities, and lead to community-level action to improve wellbeing.35 To adequately promote financial wellbeing in a way that is culturally responsive, relevant, and effective36, more robust literature is required on the specific needs and approaches to initiatives that account for complex and intersecting social locations among systemically excluded populations, as well as initiatives undertaking participatory approaches.
We found few initiatives that focused on rural populations. Living in rural communities can compound social, economic, and health inequities, including people having access to fewer employment opportunities and healthcare. One of the reviewed sourcesS5 highlighted the negative impact of pairing employment outcomes with social welfare benefits in rural Indigenous Australian communities experiencing chronic job shortages and unemployment. Socioeconomic disadvantage experienced by people who live rurally is also associated with poorer health outcomes in high-income contexts, including increased mortality. This is often attributed to decreased access to health and social services.37,38 Based on the results of our review, we suggest an increased focus on the financial wellbeing of rural communities. This should include careful consideration of structural factors such as the availability of employment opportunities and accessibility of resources and services.
Evaluating initiatives and programs is crucial to understand effectiveness, refining their delivery, and incorporating an evidence-informed approach. A source from the practice-based literature that evaluated a government-based welfare-to-work initiative for single mothers reported the negative impact of pairing employment outcomes with cash benefits.S25 This highlights the importance of evaluation and publication of the results. Nevertheless, several sources we reviewed did not undertake evaluation due to reported funding restrictionsS10,S63,S56, emphasising the need to incorporate evaluation into the initial program design.
Very few sources we reviewed evaluated the impact of policies and programs that were introduced to improve financial wellbeing and reduce financial strain in response to COVID-19. This was due to the timing of our investigation, which took place in the first year of the pandemic. Understanding the impact of these policies and practices will strengthen the evidence base for initiatives related to pandemics like COVID-19. It will also add to the literature on initiatives to promote financial wellbeing, which will be required to inform policy and programs now as many jurisdictions focus on ‘recovery’.
Limitations
To remain within the scope of a rapid review, we limited included studies by date and country. These restrictions may have introduced bias into the sources and excluded potentially relevant initiatives elsewhere. Our analysis was based on author-reported outcomes, and we did not conduct an independent review of initiative effectiveness due to the heterogeneity of studies included in the review. We acknowledge that financial strain is a prevalent and pressing issue in low- and middle-income countries that requires targeted attention. Our selection criteria was based on capturing sources that were most relevant to our research question, and captured a diversity of populations and initiatives while remaining within the scope of the rapid review. Using this purposive sampling approach may have influenced the transferability of the results.
Conclusion
We found that holistic initiatives were aligned with positive financial wellbeing and financial strain outcomes, as reported in the reviewed studies. Before targeting financial skills development, holistic initiatives ensured people’s basic needs, such as housing, food, and clothing, were met while considering SDoH, such as job opportunities. Downstream behaviour change initiatives that were not paired with wrap-around components targeting people’s basic needs were severely limited in effectiveness, as reported by reviewed studies, particularly among groups experiencing multiple forms of inequity that intersect (e.g. age, ability, and race).
We noted significant gaps in the literature related to equity. Limited initiatives included in the reviewed sources were specifically targeted and tailored for systemically excluded groups that are over-represented among people experiencing financial strain, such as racialised communities, Indigenous peoples and rural dwellers. We also identified a lack of robust evaluative data reporting the long-term impact of financial strain and financial wellbeing initiatives. More research using an equity-focused public health lens is required to understand what works for whom, how, and under what conditions to ensure an equitable approach to policy and practice to address financial wellbeing. Strong welfare and labour policies remain key to curbing increasing inequity in the present context of ‘living with COVID-19’ and its enduring physical (e.g. long-COVID) and socioeconomic effects within groups already experiencing disadvantage.39
Acknowledgements
This work was funded by the Canadian Institutes for Health Research (#172694).
We acknowledge Krystyna Kongats, Kayla Atkey, Lisa Allen Scott, Stephanie Montesanti, Jane Springett, Elaine Hyshka, Roman Pabayo, and Laura Nieuwendyk for their contributions to the research project encompassing this review. We wish to acknowledge Meghan Sebastianski (PhD) and Diana Keto-Lambert (MLIS) from the Alberta Strategy for Patient-Oriented Research (AbSPOR) SUPPORT Unit Knowledge Translation Platform for their assistance in designing and conducting the searches for the academic literature and providing guidance on the practice-based search.
Peer review and provenance
Externally peer reviewed, not commissioned.
Copyright:

© 2023 Yashadhana et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Savoy EJ, Reitzel LR, Nguyen N, Advani PS, Fisher FD, Wetter DW, et al. Financial strain and self-rated health among black adults. American J Health Behav. 2014;38(3):340–50. CrossRef | PubMed
- 2. Frank C, Davis CG, Elgar FJ. Financial strain, social capital, and perceived health during economic recession: a longitudinal survey in rural Canada. Anxiety Stress Coping.. 2014;27(4):422–38. CrossRef | PubMed
- 3. Macy JT, Chassin L, Presson CC. Predictors of health behaviors after the economic downturn: a longitudinal study. Soc Sci Med. 2013;89:8–15. CrossRef | PubMed
- 4. Kim J, Garman ET. Financial stress and absenteeism: An empirically derived research model. Financial Counseling and Planning. 2003;14(1):1–12. CrossRef
- 5. French D, Vigne S. The causes and consequences of household financial strain: A systematic review. International Review of Financial Analysis. 2019;62:150–6. CrossRef
- 6. Netemeyer RG, Warmath D, Fernandes D, Lynch Jr JG. How am I doing? Perceived financial well-being, its potential antecedents, and its relation to overall well-being. Journal of Consumer Research. 2018;45(1):68–89. CrossRef
- 7. Davis CG, Mantler J. The consequences of financial stress for individuals, families, and society. Centre for Research on Stress, Coping and Well-being Carleton University, Ottawa: Department of Psychology. 2004.
- 8. Szanton SL, Allen JK, Thorpe Jr RJ, Seeman T, Bandeen-Roche K, Fried LP. Effect of financial strain on mortality in community-dwelling older women. J Gerontol B Psychol Sci Soc Sci. 2008;63(6):S369–S74. CrossRef | PubMed
- 9. Financial Consumer Agency of Canada. Progress report: Canada's national research plan on financial literacy 2016–2018. Government of Canada; 2018 [cited 2023 May 15]. Available from: www.canada.ca/en/financial-consumer-agency/programs/research/progress-report-national-research-plan-2016-2018.html
- 10. Van Houtven CH, Friedemann-Sánchez G, Clothier B, Levison D, Taylor BC, Jensen AC, et al. Is policy well-targeted to remedy financial strain among caregivers of severely injured US service members? Inquiry. 2012;49(4):339–51. CrossRef | PubMed
- 11. Hanratty B, Holland P, Jacoby A, Whitehead M. Financial stress and strain associated with terminal cancer –a review of the evidence. Palliat Med. 2007;21(7):595–607. CrossRef | PubMed
- 12. Glenn NM, Allen Scott L, Hokanson T, Gustafson K, Stoops MA, Day B, et al. Community intervention strategies to reduce the impact of financial strain and promote financial well-being: a comprehensive rapid review. Glob Health Promot. 2021;28(1):42–50. CrossRef | PubMed
- 13. Government of Canada. The Social and Economic Impacts of COVID-19: A Six-month Update. Ottawa; Statistics Canada; 2020 [cited 2023 May 15]. Available from: www.statcan.gc.ca/en/reference/refcentre/index?MM=1
- 14. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surgery. 2020;78:185–93. CrossRef | PubMed
- 15. Glenn NM, Nykiforuk CI. The time is now for public health to lead the way on addressing financial strain in Canada. Can J Public Health. 2020;111(6):984–7. CrossRef | PubMed
- 16. Nykiforuk CIJ, Belon AP, de Leeuw E, Harris P, Allen-Scott L, Atkey K, et al. An action-oriented public health framework to reduce financial strain and promote financial wellbeing in high-income countries. Int J Equity Health. 2023;22(1):66. CrossRef | PubMed
- 17. Nykiforuk CI, Belon AP, de Leeuw E, Harris P, Allen-Scott L, Atkey K, et al. A policy-ready public health guidebook of strategies and indicators to promote financial well-being and address financial strain in response to COVID-19. Prev Chronic Dis. 2023;20:E09. CrossRef | PubMed
- 18. United Nations. World economic situation and prospects 2014: New York: United Nations Publications; 2014 [cited 2023 May 15]. Available from: www.un.org/en/development/desa/policy/wesp/wesp_current/wesp2014.pdf
- 19. Public Health Agency of Canada.Toward health equity: A tool for developing equity-sensitive public health interventions. Ottawa: PHAC; 2015 [cited 2023 May 15]. Available from: publications.gc.ca/site/eng/9.805230/publication.html
- 20. Dobbins M. Rapid review guidebook. National Collaborating Centre for Methods and Tools. Hamilton, ON: 2017.
- 21. Oliver S, Kavanagh J, Caird J, Lorenc T, Oliver K, Harden A, et al. Health promotion, inequalities and young people's health: a systematic review of research. London: EPPI-Centre University of London; 2008 [cited 2023 May 15]. Available from: discovery.ucl.ac.uk/id/eprint/1430011/
- 22. Glaser BG, Strauss AL. The discovery of grounded theory: Strategies for qualitative research. London: Routledge; 2009.
- 23. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. CrossRef | PubMed
- 24. Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Education for Information. 2018;34(4):285–91. CrossRef | PubMed
- 25. Glenn NM, Yashadhana A, Jaques K, Belon A, De Leeuw E, Nykiforuk CI, et al. The generative mechanisms of financial strain and financial well-being: a critical realist analysis of ideology and difference. Int J Health Policy Management. 2023;12(1):1–11. CrossRef
- 26. Birkenmaier J, Maynard B, Kim Y. Interventions designed to improve financial capability: A systematic review. Campbell Systematic Reviews. 2022;18(1):e1225. CrossRef | PubMed
- 27. Lorenc T, Petticrew M, Welch V, Tugwell P. What types of interventions generate inequalities? Evidence from systematic reviews. J Epidemiol Community Health. 2013;67(2):190–3. CrossRef | PubMed
- 28. Centre for Health Equity Training Research & Evaluation. Behaviour change and its per/inverse relationship with health equity. The BEE Report. Sydney; CHETRE: 2021 (No. 3) [cited 2023 May 15]. Available from: chetre.org/wp-content/uploads/2021/07/BEE_Behvioural-interventions_2021_no3.pdf
- 29. World Health Organization. Disability and health fact sheet. Geneva: WHO; 2021 [cited 2023 May 15]. Available from: www.who.int/news-room/fact-sheets/detail/disability-and-health
- 30. Kauh TJ, Read JnG, Scheitler A. The critical role of racial/ethnic data disaggregation for health equity. Populat Res Policy Rev. 2021;40(1):1–7. CrossRef | PubMed
- 31. Yashadhana A, Raven M, Pollard-Wharton N, Biles B. Aboriginal and Torres Strait Islander Peoples and the COVID-19 pandemic: a spatial and place-based analysis. The Geographies of COVID-19: Springer; 2022. p. 181–94. CrossRef
- 32. Yashadhana A, Pollard-Wharton N, Zwi AB, Biles B. Indigenous Australians at increased risk of COVID-19 due to existing health and socioeconomic inequities. Lancet Reg Health West Pac. 2020;1:1000007. CrossRef | PubMed
- 33. Parolin Z, Curran M, Matsudaira J, Waldfogel J, Wimer C. Monthly poverty rates in the united states during the COVID-19 pandemic. Poverty and social policy working paper, US: Center on Poverty & Social Policy, Columbia University; 2020 [cited 2023 May15]. Available from: www.povertycenter.columbia.edu/news-internal/2020/covid-projecting-monthly-poverty
- 34. Arriagada P, Hahmann T, O'Donnell V. Indigenous people in urban areas: Vulnerabilities to the socioeconomic impacts of COVID-19. Ottawa: Statistics Canada (Statistique Canada); 2020 [cited 2023 May 15]. Available from: www150.statcan.gc.ca/n1/en/catalogue/45280001202000100023
- 35. Salimi Y, Shahandeh K, Malekafzali H, Loori N, Kheiltash A, Jamshidi E, et al. Is community-based participatory research (CBPR) useful? A systematic review on papers in a decade. Int J Prev Med. 2012;3(6):386–93. PubMed
- 36. Bauer GR. Incorporating intersectionality theory into population health research methodology: challenges and the potential to advance health equity. Social Science & Medicine. 2014;110:10–17. CrossRef | PubMed
- 37. Cosby AG, Neaves TT, Cossman RE, Cossman JS, James WL, Feierabend N, et al. Preliminary evidence for an emerging nonmetropolitan mortality penalty in the United States. Am J Public Health. 2008;98(8):1470–2. CrossRef | PubMed
- 38. Beard JR, Tomaska N, Earnest A, Summerhayes R, Morgan G. Influence of socioeconomic and cultural factors on rural health. Aust J Rural Health. 2009;17(1):10–15. CrossRef | PubMed
- 39. de Leeuw E, Yashadhana A, Hitch D. Long-COVID: Sustained and multiplied disadvantage. Med J Aust. 2022;2016(5):222–24. CrossRef | PubMed