Abstract
Objectives: To develop a Climate Change Inequality Health Impact Assessment (CCIHIA) framework for health services; to provide a systematic process for assessing potential unequal health impacts of climate change on vulnerable and marginalised populations and places; to support effective planning to address these impacts; and to develop contextually appropriate local strategies.
Type of program: A collaborative interdisciplinary scoping research project involving two universities and two local health districts (LHDs) in New South Wales (NSW) to develop a CCIHIA framework. This work builds upon the health impact assessment (HIA) approach, which systematically assesses proposals’ potential health and equity impacts by involving stakeholders in developing responses.
Methods: The project involved four main activities: understanding stakeholder requirements; conceptualising climate change vulnerability; considering the role of health services; and integrating findings into a conceptual framework.
Results: Stakeholders identified key functions that should be addressed across the framing, process and utility of the CCIHIA framework. The resulting conceptual framework outlines contexts and social stratification, the differential impacts of climate change (including factors influencing unequal impacts) and the health system’s position, and also identifies key potential points of intervention.
Lessons learnt: The challenge of addressing the complexity of factors and resulting health impacts is reflected within the CCIHIA framework. While there are many intervention points within this framework for health services to address, many factors influencing unequal impacts are created outside the health sector’s direct control. The framework’s development process reflected the focus on collaboration and the interdisciplinary nature of climate change response. Ultimately, the CCIHIA framework is an assessment tool and an approach for prioritising inclusive, cross-cutting, multisector working, and problem-solving.
Full text
Introduction
Climate change impacts on human health, wellbeing and equity are already evident and are predicted to become more frequent and intense.1 The World Health Organization considers climate change “the biggest health threat facing humanity”.2 The impacts of climate change vary and are contextually specific to the people, places and institutions within regions. While climate change impacts everyone, the most marginalised and vulnerable in society, who are already at higher risk of poorer health outcomes, are disproportionally affected. These unequal outcomes are influenced by the quality of the urban environment and how it is used. Disadvantaged populations often reside in urban areas that are disproportionately impacted by climate change and have fewer resources available to respond to these impacts compared to areas where more advantaged populations live. This will further exacerbate health equity gaps.1,3-6
Health services play a critical role in responding to their local population’s climate change-related health needs, including the potential short- and long-term effects of climate change on health service resources, workforce and infrastructure. Local-level health services are already actively engaged in planning for and addressing the impacts of climate change on vulnerable and marginalised communities.7,8 However, much of the climate change planning and response work tends to occur in silos with particular focus areas (e.g. admissions to emergency departments (ED) from extreme heat events, decarbonisation and climate-proofing infrastructure, intersectoral collaboration with local government to support climate adaption in urban environments). While these responses are necessary, the causes and consequences of climate change impacts occur across populations and disciplinary boundaries. As the climate crisis continues to evolve, there is a need for tools and processes to systematically assess these potential impacts, take stock of and bring together existing siloed initiatives, develop responses to emergencies and support adaptation to the changing climate.
Health impact assessment (HIA) is a tool that offers the opportunity to integrate the complexity of climate change with consideration of unequal impacts across populations. HIA is a systematic process to consider a proposal’s potential health and equity impacts by involving stakeholders in systematically assessing different types of evidence and generating appropriate responses to mitigate harms and maximise benefits.9 In this way, HIA ensures that health, as understood by scientific experts, professionals and the people whose lives are affected, is considered in the planning and adaptation process.10 HIA practice is underpinned by core values of democracy, equity, sustainable development and the ethical use of evidence.9 HIA is well established in NSW through use in local health districts, universities and local councils and can be applied in diverse settings, including health services, urban planning, economic policy and advocacy.11
Against this background, our scoping project developed a Climate Change Inequality Health Impact Assessment (CCIHIA) framework to support the assessment of potential unequal health impacts of climate change on particular populations and places to inform health service responses. The purpose of the CCIHIA framework is to:
- Provide an evidence-based systematic process for health services and their key stakeholders to come together and understand how climate change has the potential to impact vulnerable and marginalised populations inequitably
- Support effective health service planning to address climate change impacts on these populations
- Support the development of contextually appropriate local strategies to address these health impacts.
The framework draws on existing conceptual frameworks and evidence and builds on previous climate change and health literature.12-18 The novel aspect of this project is the focus on the inequitable mpacts of climate change and the health services’ role and response. This paper details the processes of developing the CCIHIA framework, presents key and novel findings from the consultation process and creates a conceptual framework. The implications for both HIA practice and the resulting framework’s use are discussed.
Methods
The CCIHIA was developed in four stages. The first stage was assembling the interdisciplinary research team. The project was a collaboration between two universities (UNSW Sydney and the University of Technology Sydney) and two local health services, South Western Sydney Local Health District (LHD) and South Eastern Sydney LHD. The research team provided expertise in climate change, public health, equity and end-user perspectives to inform the framework development. In the second stage, evidence and stakeholder knowledge were collected. Key requirements for the development of CCIHIA for use in a health services setting were identified. The team conducted rapid literature reviews focusing on: the relationships between climate change and health, conceptualisations of vulnerability and inequalities, the policy environment and the role of health services. The third stage involved developing the CCIHIA framework, incorporating climate change vulnerability. In the fourth stage, the conceptual framework was reviewed by stakeholders and refined based on their feedback. At this last stage, consultation was sought with both LHD and international stakeholders identified during scoping phases as currently working in the area of climate change HIAs.
Results
A key element in ensuring the ultimate utility of the framework was consultation with stakeholders on their requirements for a CCIHIA. The requirements can be summarised into five key functions:
- Demonstrate evidence of specific climate change impacts on vulnerability and health equity
- Use both quantitative data and qualitative evidence
- Prompt health services to move beyond short-term or proximal impacts to consider longer-term structural, systemic and wider determinants of health
- Enable health services to assess both impacts on health services and on vulnerable populations
- Support the development of plans for health services to address the above impacts.
CCIHIA conceptual framework
The resulting conceptual framework guides users in considering climate change across four main areas, which come under the broader consideration of direct and indirect impacts of climate change on people, places and institutions (see Figure 1):
- Understanding existing contexts and social stratification
- Considering the differential impacts of climate change (including factors influencing climate change inequalities)
- Considering the position of the health system
- Identifying key potential points of intervention
Figure 1. Climate Change Inequality Health Impact Assessment (CCIHIA) conceptual framework
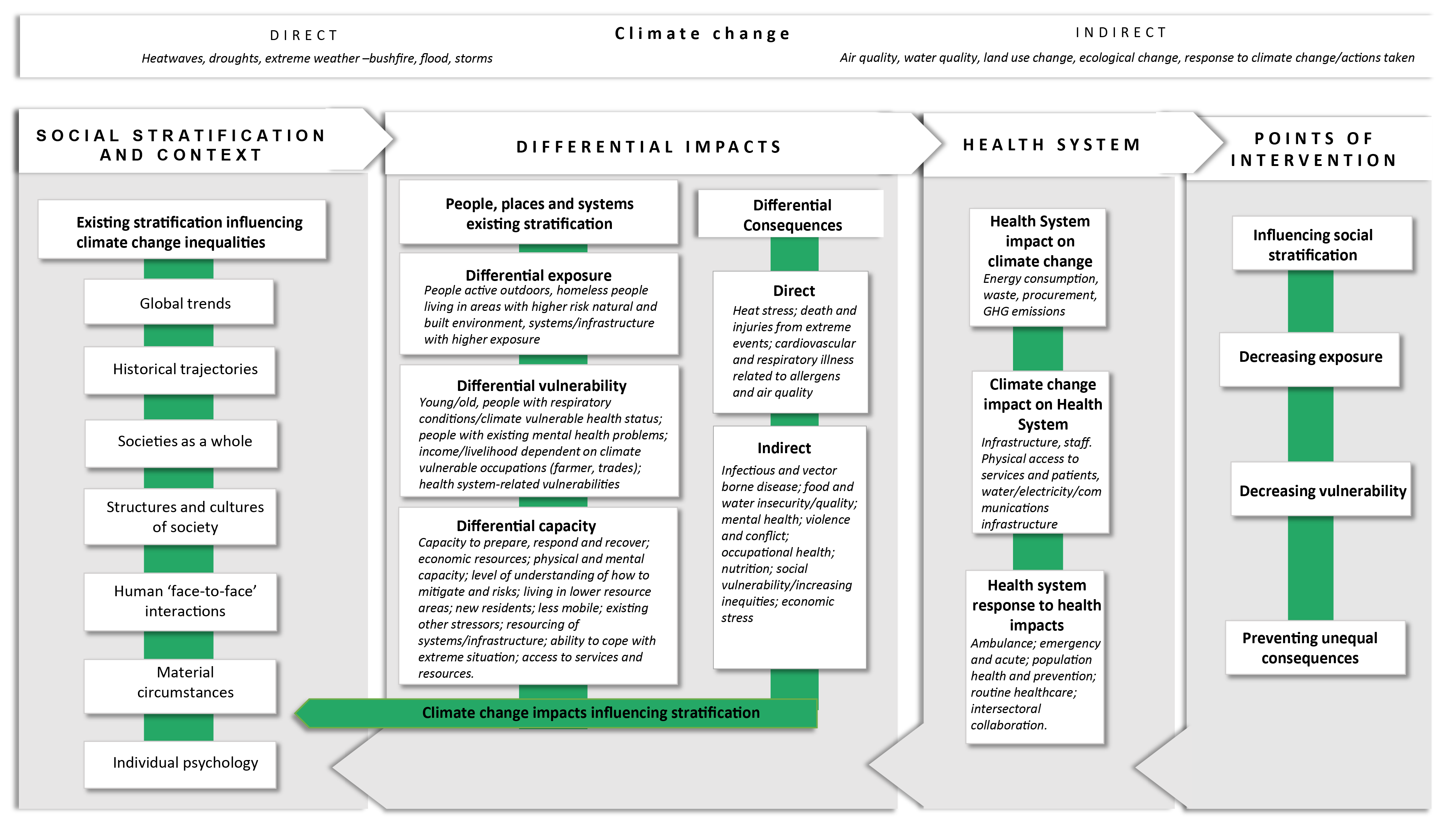
Figure 1. Climate Change Inequality Health Impact Assessment (CCIHIA) conceptual framework
The framework acknowledges that the four main areas are interrelated and may influence one another in various ways. They are situated in economic, social, political contexts and are influenced by the characteristics of people, places, institutions and systems. The framework is intended to be integrated into HIA at all stages of the process, from scoping to the generation of recommendations and reporting.
A central concept of the framework is understanding the drivers of inequalities, how these influence one another and the resulting impacts. Unequal impacts can be considered across different scales (for example global, national, regional and individual), as well as categorisations focused on the object of the unequal impact (for instance, people, systems, settings, communities and places).19 The intersectional nature of social disadvantage – in the form of existing health conditions and disability, experience of racism and discrimination, lack of income, and social isolation – also compounds vulnerability to climate change health impacts.20,21 Differential impacts within this framework are identified through the intersection of exposures, sensitivities, and capacity, aligning with the definition of vulnerability put forward by the Intergovernmental Panel on Climate Change.22
The starting point for understanding how climate change impacts health inequalities is the existing health stratification within the local population. People, places and systems have different levels of vulnerability according to their access to health determinants (stratification). Some have higher levels of exposure (direct or indirect) to climate conditions or events; others may be more sensitive to climate change through biological characteristics, resources, or infrastructure. The final type of unequal impact is particularly important, and relates to the capacity to prepare, respond to and recover from impacts. These vulnerabilities lead to differential consequences directly from climate change risks and indirectly through mitigation and adaptation measures. These unequal experiences feedback into social stratification, continuing and even exacerbating health inequities. Tailoring mitigation, adaption, and other interventions to the needs of these groups are made more difficult due to the history of stigmatisation of vulnerable populations and the further erosion of already low levels of trust in institutions and decision-making. Involving communities in assessments and understanding their experiences of health impact is a core element of HIA work.
Considering health systems and interventions
The CCIHIA conceptual framework highlights the different levels at which health services can act to reduce the inequitable impacts of climate change across the population.
These intervention points include addressing the existing causes of health inequalities (social stratification) and addressing the unequal and inequitable health outcomes resulting from climate change and responses to it. They also involve reducing the health systems’ impact on climate change and ensuring the system, services, staff, and infrastructure can continue to provide services while they are also being affected by climate change. Planning and action need to extend beyond responding to acute situations. Within a government and service framework, routine climate-related health promotion and population health approaches can and need to be developed. It is also important that health systems consider the unintended impacts of their climate response on health (e.g. stopping or limiting services during climate events). A key component of responses to health impacts is collaboration with other sectors to engage with the broader societal conditions of climate change. This includes engaging with policymakers and implementers of policy (such as local government) that shape the urban environments that are both impacted by climate change and are a key part of the response to climate change impacts. The health sector potentially has an important role in advocating for and supporting a health equity-focused response by other sectors.
The CCIHIA is not just an analytic framework or technocratic tool – rather, it demands a different approach to HIA processes and planning, in general, to focus more on differential impacts. This is achieved by involving affected groups and community organisations and using data that focuses explicitly on the distribution of effects in a disaggregated form to enable more meaningful assessment and characterisation of the impacts on the most vulnerable populations. These ways of working align with core HIA values.9
In a recent example from Wales, an HIA was carried out on climate change at a country level.23 The HIA has proven to be a beneficial process for Wales and has provided a robust evidence base that public health and health services agencies can use to mobilise action and engage with key stakeholders.23,24 Population groups identified as being unequally impacted by climate change include healthcare workforces, occupational groups such as outdoor workers, healthcare service users such as those with long-term conditions. The Welsh work has engaged stakeholders through evidence gathering and led to fruitful and long-term conversations to maximise health equity and minimise or take action on vulnerability.23,25
Conclusion
Health equity impacts often result from decisions made by organisations and people from beyond the health sector. The health system working alone cannot resolve the unequal impacts of climate change on people, places, systems and institutions. Taking action will require collaboration and partnership with other sectors and communities. While health services and healthcare professionals can be powerful advocates for change, the HIA process highlights the value of involving both communities and decision-makers when considering mitigation and reduction of climate change impacts. Public health and equity-focused tools, such as HIA, can support decision-making, stakeholder engagement and deliberate and impactful action.
Acknowledgements
We wish to acknowledge the project team and funders. Additional investigator team members:, Siggi Zapart, Kaniz Fatema, Kate Charlesworth, Brent Jacobs. Associate Investigators: Julie Dixon. Research assistance: Abela Mahimbo, Eleanor Black, Freya Sekulic, Esther Alloun, Christine Clar.
This study was funded by the Healthy Populations and Environments Platform (formerly the Healthy Urban Environments Collaboratory) within Maridulu Budyari Gumal: Sydney Partnership for Health, Education, Research and Enterprise (SPHERE).
FH report grant funding from the Healthy Urban Environments 2020 Seed Funding Scheme. JP and BHR report grant funding from SPHERE.
This paper is part of a special issue of the journal focusing on urban planning and development for health, which has been produced in partnership with the Healthy Populations and Environments Platform, SPHERE. JP was a guest editor for the special issue. He was not involved in the review of or decisions on this manuscript.
Peer review and provenance
Externally peer reviewed, invited.
Copyright:

© 2023 Haigh et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Watts N, Amann M, Ayeb-Karlsson S, Belesova K, Bouley T, Boykoff M, et al. The Lancet Countdown on health and climate change: from 25 years of inaction to a global transformation for public health. Lancet. 2018;391(10120):581–630. CrossRef | PubMed
- 2. World Health Organization. Climate change and health. Geneva: WHO; 2018 [cited 2023 Sep 12]. Available from: www.who.int/news-room/fact-sheets/detail/climate-change-and-health
- 3. Kinney PL. Interactions of climate change, air pollution, and human health. Curr Environ Health Rep. 2018;5(1):179–86. CrossRef | PubMed
- 4. Bambrick HJ, Capon AG, Barnett GB, Beaty RM, Burton AJ. Climate change and health in the urban environment: adaptation opportunities in Australian cities. Asia Pac J Public Health. 2011;23(2 Suppl):67S–79. CrossRef | PubMed
- 5. Kjellstrom T, Gabrysch S, Lemke B, Dear K. The ‘Hothaps’ programme for assessing climate change impacts on occupational health and productivity: an invitation to carry out field studies. Glob Health Action. 2009;2(1):2082. CrossRef | PubMed
- 6. Green D. Climate change and health: impacts on remote Indigenous communities in Northern Australia. Victoria: CSIRO Marine and Atmospheric Research; 2006 [cited 2023 Sep 12]. Available from: citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.553.1262&rep=rep1&type=pdf
- 7. Rychetnik L, Sainsbury P, Stewart G. How Local Health Districts can prepare for the effects of climate change: an adaptation model applied to metropolitan Sydney. Aust Health Rev. 2019;43:601–610. CrossRef | PubMed
- 8. Charlesworth KE, Jamieson M. Healthcare in a carbon-constrained world. Aust Health Rev. 2019;43(3):241–5. CrossRef | PubMed
- 9. European Centre for Health Policy. Gothenburg consensus paper: health impact assessment.Main concepts and suggested approach. Brussels: ECHP; 1999 [cited 2023 Sep 12]. Available from: www.healthedpartners.org/ceu/hia/hia01/01_02_gothenburg_paper_on_hia_1999.pdf
- 10. Chadderton C, Elliott E, Hacking N, Shepherd M, Williams G. Health impact assessment in the UK planning system: the possibilities and limits of community engagement. Health Promot Int. 2012 Jul 15;28(4):533–43. CrossRef | PubMed
- 11. Haigh F, Baum F, Dannenberg A, Harris M, Harris-Roxas B, Keleher H, et al. The effectiveness of health impact assessment in influencing decision-making in Australia and New Zealand 2005–2009. BMC Public Health. 2013;13(1):1188–97. CrossRef | PubMed
- 12. Blashki G, Armstrong G, Berry HL, Weaver HJ, Hanna EG, Bi P, et al. Preparing health services for climate Change in Australia. Asia Pac J Public Health. 2011;23(2):133S–143S. CrossRef | PubMed
- 13. Spickett JT, Brown HL, Katscherian D. Adaptation strategies for health impacts of climate change in Western Australia: Application of a Health Impact Assessment framework. Environ Impact Assess Rev. 2011 Apr 1;31(3):297–300. CrossRef
- 14. Brown HL, Proust K, Spickett J, Capo A. The potential role of health impact assessment in tackling the complexity of climate change adaptation for health. Health Promot J Aust 2011;22 Spec No:S48–53. CrossRef | PubMed
- 15. Patz J, Campbell-Lendrum D, Gibb H, Woodruff R. Health impact assessment of global climate change: expanding on comparative risk assessment approaches for policy making. Annu Health. 2008;29:27–39. CrossRef | PubMed
- 16. Brown H, Spickett J, Katscherian D. A health impact assessment framework for assessing vulnerability and adaptation planning for climate change. Int J Environ Res Public Health. 2014;11(12):12896–914. CrossRef | PubMed
- 17. Boylan S, Beyer K, Schlosberg D, Mortimer A, Hime N, Scalley B, et al. A conceptual framework for climate change, health and wellbeing in NSW, Australia. Public Health Res Pract. 2018;28(4):e2841826. CrossRef | PubMed
- 18. Hime N, Vyas A, Lachireddy K, Wyett S, Scalley B, Corvalan C. Climate change, health and wellbeing: challenges and opportunities in NSW, Australia. Public Health Res Pract. 2018;28(4):e2841824. CrossRef | PubMed
- 19. Adapt NSW. Climate change impact on heatwaves. Sydney: NSW Government; 2023 Nov [cited 2023 Sep 12]. Available from: climatechange.environment.nsw.gov.au/Impacts-of-climate-change/Heat/Heatwaves
- 20. Bowleg L. We’re not all in this together: on COVID-19, intersectionality, and structural inequality. Am J Public Health. 2020;110(7):917. CrossRef | PubMed
- 21. Osborne N. Intersectionality and kyriarchy: A framework for approaching power and social justice in planning and climate change adaptation. Plan Theory. 2015;1;14(2):130–51. CrossRef
- 22. Intergovernmental Panel on Climate Change. Climate Change 2007: impacts, adaptation and vulnerability. New York, US: Cambridge University Press; 2007 [cited 2023 Sep 12]. Available from: www.ipcc.ch/site/assets/uploads/2018/03/ar4_wg2_full_report.pdf
- 23. Green L, Edmonds N. Climate change in Wales and its health impact: who is vulnerable and how? Eur J Public Health. 2021;31(Supplement_3):ckab164.024. CrossRef
- 24. Green L, Ashton K, Azam S, Clemens T, Bellis M. Brexit, COVID-19 and climate change: mapping the impact of the ‘triple challenge’ on health and well-being in Wales. Impact Assess Proj Apprais. 2023;41(2):126–38. CrossRef
- 25. Edmonds N, Green L. Climate change in Wales: Health Impact Assessment. Summary report. Public Health Wales, NHS Trust; 2023 [cited 2023 Oct 17]. Available from: phwwhocc.co.uk/wp-content/uploads/2023/07/PHW-Climate-Change-HIA-Summary-Report-E-17_07-FINAL-1300.pdf