Full text
Introduction
Dementia is associated with a decline in cognition and daily function, presenting with related symptoms such as memory impairment and problems with speech, movement or mobility.1 It affects approximately 487 500 Australians and is predicted to affect >1.1 million by 2058.2 The annual care costs are estimated to increase from $9.1 billion in 2017 to A$24.1 billion by 2056.3
Currently, there is a lack of a single valid and reliable data source for dementia identification. Welberry et al. recently demonstrated the feasibility of linking large population-based cohorts to administrative datasets to identify dementia cases at different stages of their trajectory.4
The Addressing Dementia Through Analysis of Population Traits and Risk Factors (ADAPTOR) project links data from a large Australian cohort study (followed up for 15 years) to various administrative health datasets. While the project links the same cohort study (the Sax Institute’s 45 And Up Study) and administrative datasets for dementia identification, it expands on Welberry et al.’s study by extending the data cut-off period from June 2014 to June 2018; including additional datasets and participants aged between 45–54 years; and stratifying data by sex and age group. The ADAPTOR project estimates dementia incidence, investigates the association between risk factors and incidence, and models the impact of modifiable risk factor reduction (e.g. increased physical activity, reduced alcohol consumption) on population-level dementia incidence. This paper presents preliminary findings from the project on sex and age-specific incidence of dementia and presents the most common data sources for dementia identification.
Methods
The ADAPTOR project used data from the 45 and Up Study (hereafter referred to as the Study) of >267 357 New South Wales residents aged ≥45 years, randomly sampled from the Services Australia Medicare enrolment database.5 Participants aged 80 years and older and residing in rural/remote areas were overrepresented in the sample. There were a small number (<1%) of volunteer participants.5 Unique Project Person Numbers from participants were linked to multiple administrative datasets containing information relevant to dementia identification. Linked datasets included the Pharmaceutical Benefits Scheme, Emergency Department Data Collections, Admitted Patients Data Collections, Cause of Death, Mental Health Ambulatory data, Aged Care Assessment Program, Aged Care Funding Instrument data and Home Care Package- Entry (see Supplementary Table 1, available from: figshare.com/s/7dec7363115708f521b1).
Ethics
Ethical approval was obtained from the New South Wales Population and Health Service Research Ethics Committee (2019/ETH00118) and Australian Institute of Health and Welfare Ethics Committee (EO2019/4/1062).
Dementia identification
Dementia cases were identified following previous approaches4 (codes and variables in Supplementary Table 1, available from: figshare.com/s/7dec7363115708f521b1). Participants were considered to have a dementia diagnosis if they had a relevant record in one of the linked datasets; this included the first indication of dementia in the Cause of Death records. The earliest date recorded across the data sources was considered the onset date. Prevalent cases, i.e., cases diagnosed two years prior to recruitment to the Study, were excluded.
Study period
The study period commenced with enrolment to the 45 and Up Study (between February 2006 and December 2009) and ended on 30 June 2018. Earliest records available in all administrative datasets are from before or during enrolment to the Study, while dates of the last records varied (see Supplementary Figure 1, available from: figshare.com/s/7dec7363115708f521b1).
Statistical methods
The proportion of incident cases were identified in each data source, and the five most common combinations of data sources were tabulated (as people could be identified in multiple sources).
Dementia incidence rates were produced by dividing the number of incident cases by the number of person-years of follow-up. Person years were the years between enrolment and the end of the follow-up period, or the first identified date of dementia or death (whichever came first). Incidence rates were calculated with 95% Confidence Intervals (CIs), stratified within sex and 5-year age groups (e.g., 45–49, 50–54, 55–59 etc.). For each age group, differences in incidence rates between males and females were tested with a Poisson regression approach.
Results
Participants
Of the 265 150 eligible participants in the Study, 1 541 prevalent dementia cases were excluded, leaving a final cohort of 263 609 participants. More than half (54%) of the participants were female, and 62% were aged between 45–64 years at recruitment. The number of participants per strata ranged from 20 434 (8%) for females aged 75 years and older to 92 920 (35%) for females between 45–64 years.
In the final cohort in this analysis, 15 224 incident dementia cases were identified; the highest proportion were identified in the Hospital Admitted Patients Data Collection and the Aged Care Funding Instrument data sources (60% identified in each data set). The majority of dementia cases (62%) were identified in two or more data sources.
Figure 1. Number of dementia cases per 1000 person-years and 95% confidence intervals per 5-year age group and sex (click figure to enlarge)
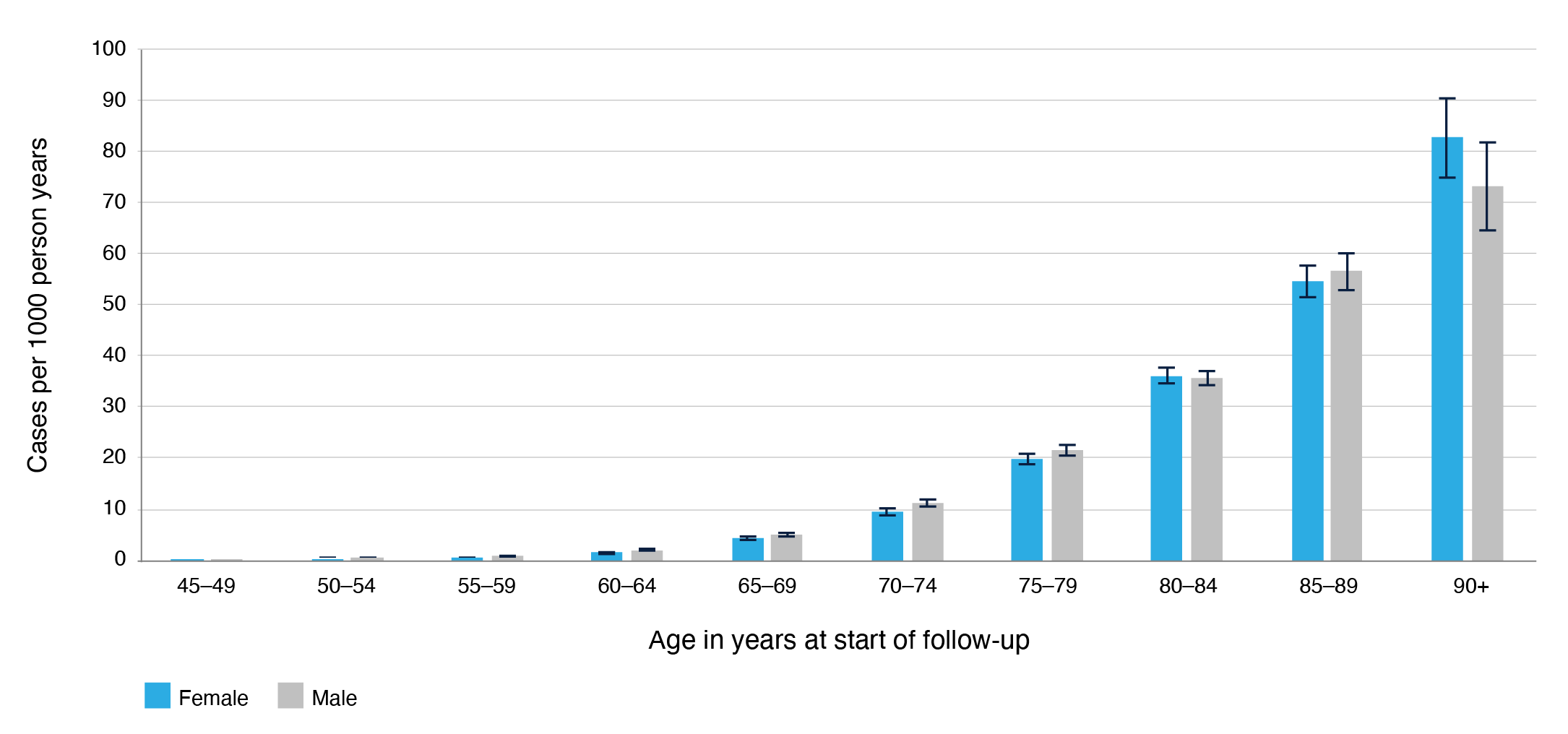
Incidence rates among females ranged from 0.14 cases per 1 000 person-years (95% CI: 0.1, 0.2) in those aged 45–49 years to 82.62 cases per 1 000 person-years (95 CI: 74.80, 91.26) among those aged 90 years and older (Figure 1). Incidence rates among males ranged from 0.27 cases per 1 000 person-years (95% CI: 0.19, 0.37) in 45–49-year-olds to 73.11 cases per 1 000 person-years (95% CI: 64.36, 83.05) among those aged 90 years and older (see Supplementary Table 2, available from figshare.com/s/7dec7363115708f521b1). Incidence rates were higher among males than females for the following age groups: 50–54, 55–59, 60–64, 65-69 and 70–74 (p-value <0.01). In the remaining age groups (80-84, 85-89 and 90+), the difference in incidence between males and females was not significant (See Supplementary Table 2, available from: figshare.com/s/7dec7363115708f521b1).
Discussion and conclusion
The findings from the ADAPTOR project confirm that dementia incidence increases substantially with age. Incidence rates ranged between 0.14–82.62 cases per 1 000 person-years (females) and 0.27–73.11 cases per 1 000 person-years (males). In the majority of age groups, the rates were higher in males than females. Most dementia cases were identified in two or more data sources.
The longer follow-up period and additional datasets in the ADAPTOR project, compared to Welberry et al. have led to the identification of more than 9000 additional dementia cases in this cohort. Relatedly, dementia incidence per 1 000 person-years, age-stratified incidence rate ratios, and incidence rates in those aged <59 year olds were found to be higher in the current project.
The main strength of the ADAPTOR project is the linkage of multiple administrative data sources to a large cohort, allowing dementia identification through multiple sources. The large cohort will enable findings to be used for population-level estimates, subpopulation comparisons, understanding trends, and capturing data from participants with cognitive decline or lost to follow-up.
A limitation of using administrative datasets is that diagnoses are only captured for people accessing or claiming services/medications. Another limitation is the selection bias due to low participation rate (19%), over representation of population subgroups, and voluntary participation in the Study. Factors correlated with service use and selection bias need to be considered when interpreting results.
Findings from the ADAPTOR project strengthen the evidence on using multiple data linkage in dementia identification. The project informs dementia epidemiology by expanding dementia identification approaches that can consequently inform its prevention and management. In the absence of curative treatment options, improving dementia diagnosis (including early diagnosis) can delay disease progression by allowing patients to seek treatment earlier in the course of the disease.
Acknowledgements
Funding for this research was provided by the Australian Government Medical Research Future Fund (MRFF), through the Australian Prevention Partnership Centre. KA is funded by ARC Fellowship FL190100011. HW is part funded by NHMRC Grant #1171279. The 45 and Up Study is managed by the Sax Institute in collaboration with partners Cancer Council NSW, the Heart Foundation and NSW Ministry of Health.
Peer review and provenance
Externally peer reviewed, not commissioned.
Competing interests
AG reports receiving payment for educational presentations from the National Ageing Research Institute and Hammond Care. HB reports Board memberships for Roche, Skin2Neuron, Cranbrook Care, Montefiore Homes and a consultancy for Biogen. KA reports receiving a symposium presenter fee from Nutricia.
Author contributions
SN led the manuscript preparation and was responsible for editing the manuscript. XDG, DC and CE were responsible for study design, data analysis and assisted in manuscript preparation. KA, HB, HW and AG provided expert input on dementia and analytical advice. MM was responsible for project supervision, reviewing and editing the manuscript.
Copyright:

© 2023 Smriti et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Chertkow H, Feldman HH, Jacova C, Massoud F. Definitions of dementia and predementia states in Alzheimer's disease and vascular cognitive impairment: consensus from the Canadian conference on diagnosis of dementia. Alzheimers Res Ther. 2013;5(Suppl 1):S2. CrossRef | PubMed
- 2. Dementia Australia. Dementia statistics. Australia: Dementia Australia; 2022-Updated January 2022. [cited 2023 Mar 23]. Available from: www.dementia.org.au/sites/default/files/2021-03/2021-Dementia-Key-Facts-Stats.pdf
- 3. Brown L, Hansnata E, La HA. Economic cost of dementia in Australia 2016–2056. Australia: Alzheimer’s Australia; 2017 [cited 2023 Mar 23]. Available from: www.dementia.org.au/sites/default/files/NATIONAL/documents/The-economic-cost-of-dementia-in-Australia-2016-to-2056.pdf
- 4. Welberry HJ, Brodaty H, Hsu B, Barbieri S, Jorm LR. Measuring dementia incidence within a cohort of 267,153 older Australians using routinely collected linked administrative data. Sci Rep. 2020;10(1):8781. CrossRef | PubMed
- 5. Bleicher K, Summerhayes R, Baynes S, Swarbrick M, Navin Cristina T, Luc H, et al. Cohort Profile Update: The 45 and Up Study. Int J Epidemiol. 2023; 52(1):e92–101. CrossRef | PubMed