Abstract
The incidence of skin cancer, including melanoma, continues to climb in white populations around the world, imposing a large and growing burden on health systems and individuals. Harmful exposure to ultraviolet (UV) radiation, mostly solar UV, is the most avoidable cause of skin cancer risk and mortality. Many economic evaluations attest to the favourable benefits for governments and citizens from skin cancer prevention programs. This overview presents the current ‘state of play’ of the economics of skin cancer prevention. More research is required to document contemporary costs of managing skin cancer in Australia and New Zealand to accurately assess the true savings from primary prevention. New directions are proposed for ways that economics could contribute to the investment case for prevention. The majority of skin cancers are avoidable and curable, yet cost the Australian health economy A$1.7 billion each year. Therefore primary prevention of skin cancers must remain high on the public health agenda.
Full text
Primary prevention: a priority for health investment
Healthcare costs for cancers are rapidly increasing, creating the urgent need for cancer prevention programs that spend wisely on cost-effective preventive interventions. Although melanoma is the most serious form of skin cancer and receives significant attention among clinicians and researchers, the sheer volume of the more common keratinocyte cancers means that estimated health expenditure in Australia for these skin lesions alone (A$1.3 billion in 2018–19) dwarfs that for melanoma (A$0.4 billion) – total costs are A$1.7 billion.1 This paper reports on our contemporary understanding of the economic burden of skin cancer and highlights the benefits of primary prevention as a priority for health investment.
Cost effectiveness of skin cancer prevention
In a 2015 review of the economic evidence regarding skin cancer burden and prevention2, six comprehensive economic evaluations in multiple countries found prevention programs, including SunSmart programs, school-based initiatives, and promoting regular sunscreen use, were either cost-saving or cost-effective. Nine studies across Australasia, Europe and North America reported national cost-of-illness findings (i.e., reports that identify and measure the broad costs of a particular disease) and four studies reported simple analyses of melanoma screening.2 Since 2015, attention has switched to health economic analyses of improved screening programs but with mixed findings, even among those targeting sub-populations at higher risk than the general population.3-6 On the other hand, several cost-effectiveness studies of primary prevention interventions in general populations3,5,6 including two Australian studies7,8 showed them to be highly cost-effective: for every dollar or Euro spent on skin cancer prevention, the return on investment was 2–4 times greater.7,8
Cost-effectiveness studies on sunbed regulations add to the favourable economic and health evidence for primary prevention. After the 2009 International Agency for Research on Cancer statement of indoor tanning carcinogenicity, sunbed use dramatically reduced worldwide between 2007–2012 and 2013–2018 in adolescents (22.0% to 6.5%) and adults (18.2% to 10.4%).9 Long-term health system cost savings and productivity benefits were estimated to be 3-fold higher for a complete ban of commercial sunbeds, such as in Australia, versus banning use in minors only.10
Only one study has compared the economic trade-offs between early detection and primary prevention in general populations.11 Although early detection remains important for preventing skin cancers in high-risk individuals (e.g. organ transplant recipients, those with personal history of melanoma or genetic predisposition5), primary prevention in the form of regular sun-protection use was superior for the general population of Australia, reducing the development of skin cancers and avoiding resource use for mass screening and over-diagnosis.11,12
Benefits and challenges with costing studies
Advances in data linkage and simulation modelling have improved the quality and breadth of cost-effectiveness analyses.6 However, studies vary widely, differing in perspective (societal vs health system) and scope where, for example, some economic studies include melanomas only3 while others cover all skin lesions treated.13 Some prevention programs evaluated were population-based, taking a whole-system approach, while others were single interventions. Despite surveillance being included, many analyses have excluded the commonly occurring multiplicity of keratinocyte cancers and melanomas in individuals, or new systemic drugs being used as adjuvant or advanced melanoma therapies. Indeed all cost-of-illness studies are somewhat outdated as they have omitted the high costs of rapidly changing advanced melanoma therapies. Nevertheless, since the vast majority of all skin cancers are preventable by reducing exposure to UV radiation, these aggregated national costs present the potential cost-savings from preventive strategies.
A challenge with costing studies in Australia and New Zealand is capturing data at the general practice level where most skin cancer is managed. Little is known about costs related to screening and management in general practice, the numbers detected in routine skin checks versus opportunistic screening, diagnostic accuracy and consequences of false positives, and of incidental findings, the role played by skin cancer clinics versus generalist practices, the use of dermoscopy training in general practice and the costs of different treatment options/pathways. Data linkage of a dedicated general practice–generated dataset (e.g. The Bettering the Evaluation and Care of Health [BEACH] national study of general practitioner clinical activity; the POpulation Level Analysis and Reporting [POLAR] general practice database and NPS MedicineWise’s MedicineInsight program) with administrative datasets (e.g. Medicare, cancer registry) would greatly assist in future cost-of-illness research. Moreover, the burden on public hospitals of skin cancer treatment and management cannot be overlooked14, and was estimated in 2012–13 at about $50 million per year in the state of Victoria alone.
Economic impact of new treatments
Further studies are needed to reflect the contemporary costs of skin cancer especially with ageing populations and management changes for late-stage melanomas. Trials are underway in stage II melanoma and advanced keratinocyte cancers for immunotherapies, reflecting the incentive to optimise treatment at earlier stages of disease, albeit placing continued pressure on the public purse. A systematic review by Gorry et al. in 2020 revealed 15 studies on the cost-effectiveness of advanced melanoma treatments, many sponsored by industry.15 Ipilimumab was the first immunotherapy to be listed on drug formularies around the world and controversially, created a high benchmark for determining the cost of subsequent therapies during health technology assessments. None of the new therapies for advanced melanoma are cost-effective compared with previous standard chemotherapy (dacarbazine) and generally, are only funded in wealthy countries.15
Government spending on skin cancer
In Australia and New Zealand, the two countries with the highest skin cancer burden in the world, there has been no national investment in skin cancer prevention for over a decade.16 By comparison, spending by the Australian Government on systemic therapies for melanoma is extensive, and was $499.2 million in 2020–21 for seven drugs used to treat advanced melanoma (Figure 1). Nivolumab is currently the predominant therapy used and has the highest overall government cost for both unresectable and resectable stage III and IV disease. In stark contrast, the predicted investment in skin cancer prevention of $62 million over 20 years ($3.1 million per year) from 2011 to 2030 could achieve a $3.20 return for every dollar invested.8
Figure 1. Australian Government benefits paid on the Pharmaceutical Benefits Scheme for advanced stage melanoma therapies 2020–21 financial year (click to enlarge)
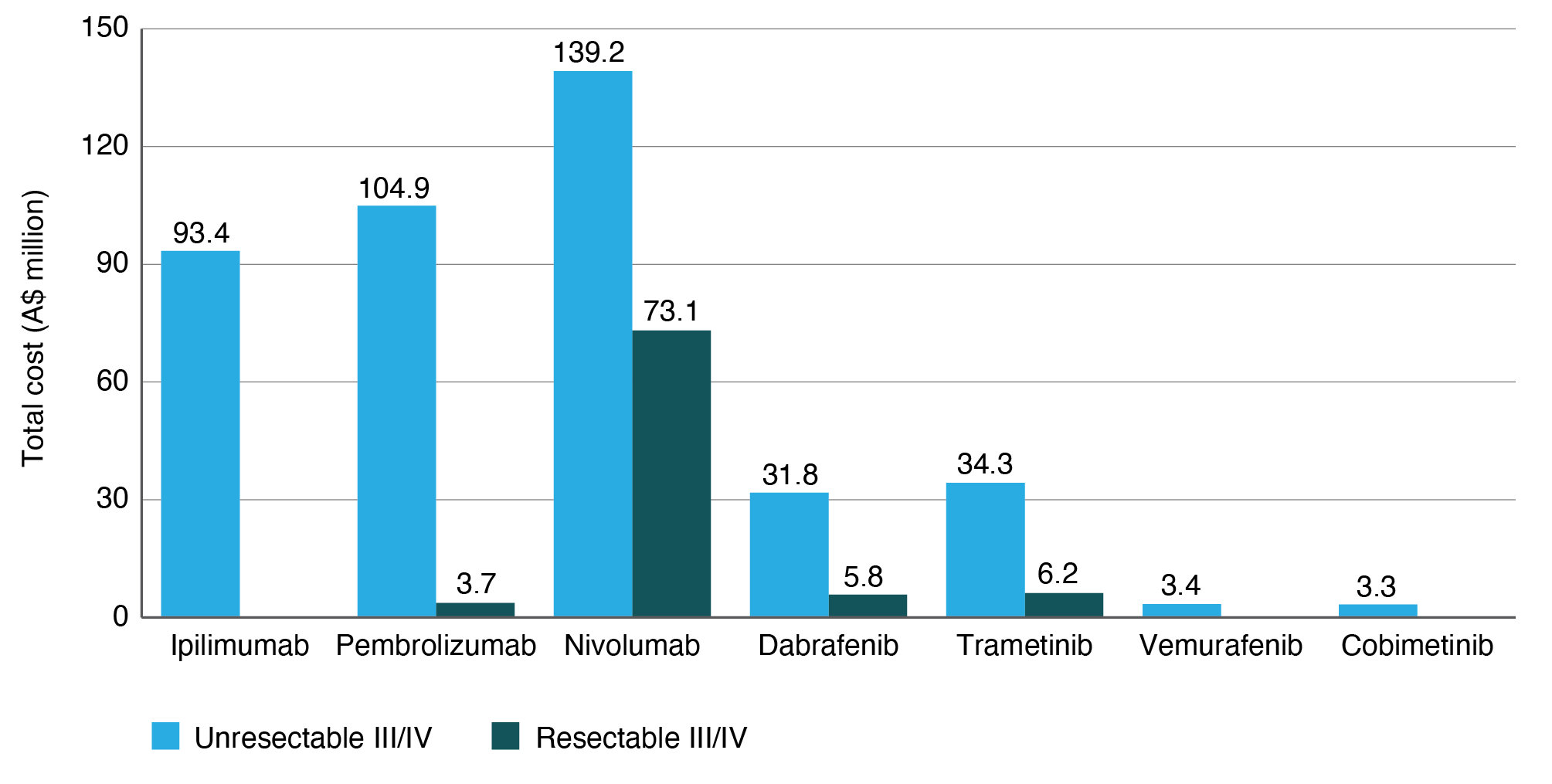
Source: PBS item reports (item numbers: 2638W, 2641B, 2963Y, 2846T, 2954L, 10003L, 10475H, 10493G, 10424P, 10436G, 12122B, 12123C, 12124D, 12128H, 10403M, 10382K, 10385N, 10405P, 10775D, 10764M, 10745M, 10748Q, 11532Y, 11543M, 11074W, 11075X, 11076Y, 11081F, 11823G, 11820D, 12125E, 12127G, 12130K, 12120X, 11821E, 11819C, 11906P, 11900H. Includes all initial and continuing scripts). medicarestatistics.humanservices.gov.au/statistics/pbs_item.jsp
Workplace policies
Institutional policies for prevention are potentially strong forces for prevention and more studies are needed to assess cost-effectiveness for workplace shade and personal protective wear17, school-based protective clothing18 and other policies. Economic studies on the financial burdens to patients, families and individuals affected by skin cancers would also be valuable to highlight the growing out-of-pocket costs for medical care and time off work. Increased time devoted to disseminating economic evidence, often highly technical and jargon laden, may also be valuable, as well as working with advocates and decision makers to strengthen the case for investing in skin cancer prevention. There is also an increasing role of behavioural economic approaches for health promotion and healthy behaviour change.19 Supported by studies in consumer preferences around early detection and teledermoscopy (i.e., sending images of skin lesions to a clinician for diagnosis)20, these approaches will improve feasibility of new programs with strong consumer engagement and may lower consumer expenses.21
Workplace incentives such as providing free sunscreen or tax deductions for purchasing sunscreen would be likely to motivate individuals to engage in more sun protection. Sunscreens are sold widely throughout Australia at increasing retail value, yet each year, only 0.17 litres per capita are currently consumed (equivalent to 33 teaspoons of sunscreen each year, where one teaspoon will protect just one limb for 2 hours) (Figure 2). This consumption is grossly inadequate given that average UV Index annual values for mainland Australia range from high to extreme.22 Government regulation to reduce the prices of approved sunscreen products and other protective equipment would increase general access to sun protection. Different payment models such as value-based care payments (rather than fee for service) or bundled care packages for skin cancer management could also be evaluated and may provide different incentives for GPs to improve patient outcomes. Ultimately, successful approaches to prevention as a coordinated set of skin protection activities should make it easier for individuals to reduce their exposure to UV radiation.
Figure 2. Sunscreen market in Australia from 2006 to 2025 (projected) by retail value and volume (click to enlarge)
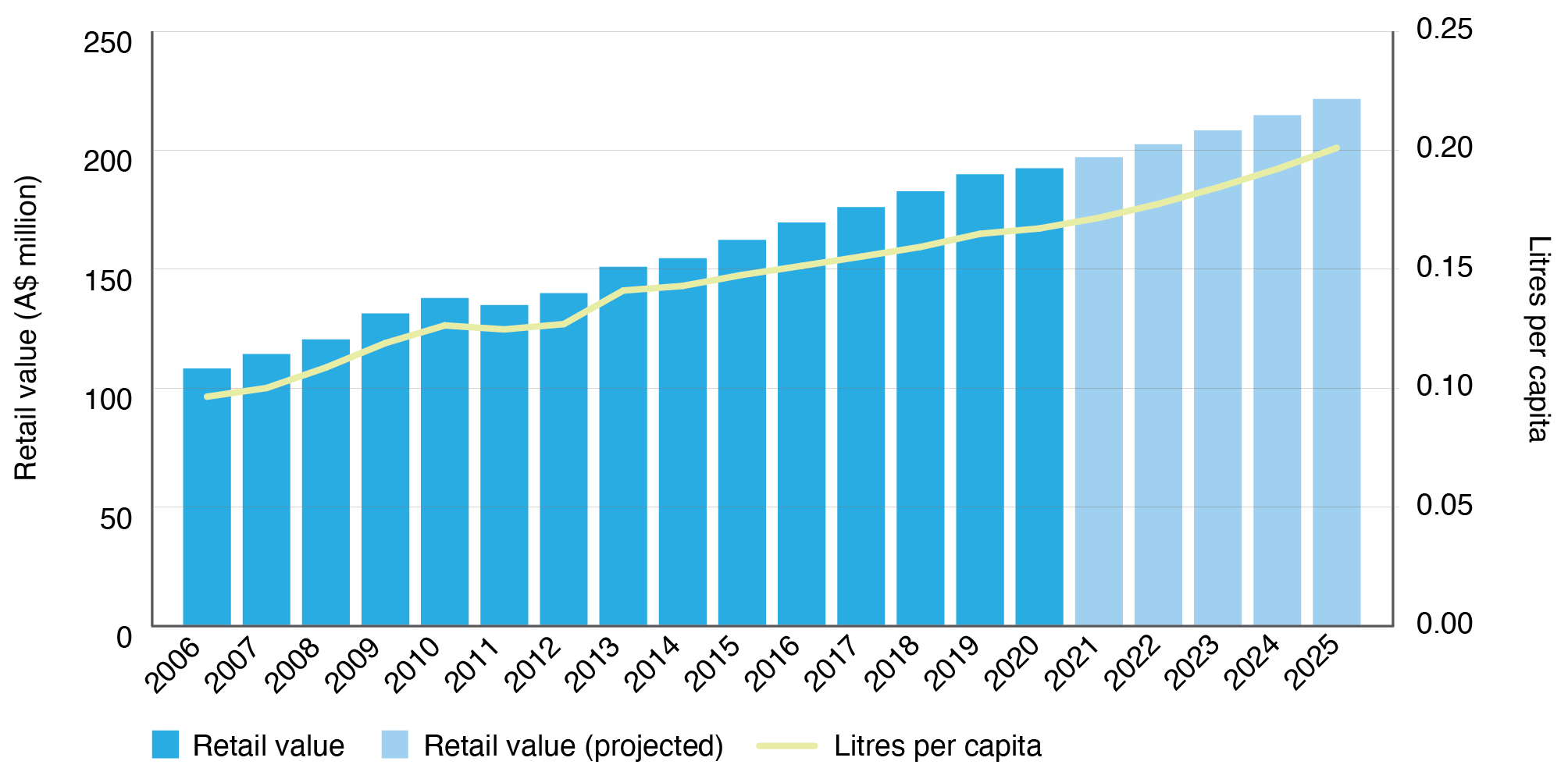
Source: Euromonitor International ‘Sun Care in Australia’ report extracted on 29 April 2021.
Conclusion
More and higher-quality evidence has evolved over time showing the economic benefits of primary prevention of skin cancer, but further studies are needed. Economic research should be directed at evaluating organisational policies, different payment models, financial incentives to promote sun protection and policies to lower costs in sun-protection markets (e.g. sunscreen) to improve access and uptake. Cost-of-illness studies are needed to monitor the rising costs of skin cancers and to highlight to policy makers the relatively high return on investment for prevention versus high-cost treatment.
Peer review and provenance
Externally peer reviewed, invited.
Copyright:

© 2021 Gordon et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Australian Institute of Health and Welfare. Disease expenditure in Australia 2018–19. Canberra: AIHW; 2021 [cited 2021 Dec 13]. Available from: www.aihw.gov.au/getmedia/9ce5ae2a-f574-4089-8d52-158abb4bdb09/Disease-expenditure-in-Australia-2018-19.pdf.aspx?inline=true
- 2. Gordon LG, Rowell D. Health system costs of skin cancer and cost-effectiveness of skin cancer prevention and screening: a systematic review. Eur J Cancer Prev. 2015;24(2):141–9. CrossRef | PubMed
- 3. Buja A, Rivera M, Girardi G, Vecchiato A, Rebba V, Pizzo E, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27(3):157–67. CrossRef | PubMed
- 4. Podlipnik S, Moreno-Ramirez D, Carrera C, Barreiro A, Manubens E, Ferrandiz-Pulido L, et al. Cost-effectiveness analysis of imaging strategy for an intensive follow-up of patients with American Joint Committee on Cancer stage IIB, IIC and III malignant melanoma. Br J Dermatol. 2018;7(10):16833. CrossRef | PubMed
- 5. Watts CG, Cust AE, Menzies SW, Mann GJ, Morton RL. Cost-effectiveness of skin surveillance through a specialized clinic for patients at high risk of melanoma. J Clin Oncol. 2017;35(1):63–71. CrossRef | PubMed
- 6. Wilson ECF, Usher-Smith JA, Emery J, Corrie P, Walter FM. A modeling study of the cost-effectiveness of a risk-stratified surveillance program for melanoma in the United Kingdom. Value Health. 2018;21(6):658–68. CrossRef | PubMed
- 7. Doran CM, Ling R, Byrnes J, Crane M, Shakeshaft AP, Searles A, et al. Benefit cost analysis of three skin cancer public education mass-media campaigns implemented in New South Wales, Australia. PLoS One. 2016;11(1):e0147665. CrossRef | PubMed
- 8. Shih ST, Carter R, Heward S, Sinclair C. Economic evaluation of future skin cancer prevention in Australia. Prev Med. 2017;99:7–12. CrossRef | PubMed
- 9. Rodriguez-Acevedo AJ, Green AC, Sinclair C, van Deventer E, Gordon LG. Indoor tanning prevalence after the International Agency for Research on Cancer statement on carcinogenicity of artificial tanning devices: systematic review and meta-analysis. Br J Dermatol. 2020;182(4):849–59. CrossRef | PubMed
- 10. Gordon LG, Rodriguez-Acevedo AJ, Køster B, Guy GP Jr, Sinclair C, Van Deventer E, et al. Association of indoor tanning regulations with health and economic outcomes in North America and Europe. JAMA Dermatol. 2020;156(4):401–10. CrossRef | PubMed
- 11. Gordon LG, Olsen C, Whiteman DC, Elliott TM, Janda M, Green AC. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10(2):1–13. CrossRef | PubMed
- 12. Glasziou PP, Jones MA, Pathirana T, Barratt AL, Bell KJ. Estimating the magnitude of cancer overdiagnosis in Australia. Med J Aust. 2020;212(4):163–8. CrossRef | PubMed
- 13. Anderson A, Matsumoto M, Secrest A, Saul MI, Ho J, Ferris LK. Cost of treatment of benign and premalignant lesions during skin cancer screening. JAMA Dermatol. 2021;157(7):876–9. CrossRef | PubMed
- 14. Shih STF, Carter R, Heward S, Sinclair C. Skin cancer has a large impact on our public hospitals but prevention programs continue to demonstrate strong economic credentials. Aust N Z J Public Health. 2017;41(4):371–6. CrossRef | PubMed
- 15. Gorry C, McCullagh L, Barry M. Economic evaluation of systemic treatments for advanced melanoma: a systematic review. Value Health. 2020;23(1):52–60. CrossRef | PubMed
- 16. Walker H, Maitland C, Tabbakh T, Preston P, Wakefield M, et al. Forty years of Slip! Slop! Slap! A call to action on skin cancer prevention for Australia. Pub Health Res Prac. 2021; Online early publication: e31452117. CrossRef
- 17. Mofidi A, Tompa E, Song C, Tenkate T, Arrandale V, Jardine KJ, et al. Economic evaluation of interventions to reduce solar ultraviolet radiation (UVR) exposure among construction workers. J Occup Environ Hyg. 2021;18(6):250–64. CrossRef | PubMed
- 18. Kyle JW, Hammitt JK, Lim HW, Geller AC, Hall-Jordan LH, Maibach EW, et al. Economic evaluation of the US Environmental Protection Agency's SunWise program: sun protection education for young children. Pediatrics. 2008;121(5):e1074–84. CrossRef | PubMed
- 19. Vlaev I, King D, Darzi A, Dolan P. Changing health behaviors using financial incentives: a review from behavioral economics. BMC Public Health. 2019;19(1):1059. CrossRef | PubMed
- 20. Spinks J, Janda M, Soyer HP, Whitty JA. Consumer preferences for teledermoscopy screening to detect melanoma early. J Telemed Telecare. 2016;22(1):39–46. CrossRef | PubMed
- 21. Wang RH, Barbieri JS, Nguyen HP, Stavert R, Forman HP, Bolognia JL, et al. Clinical effectiveness and cost-effectiveness of teledermatology: where are we now, and what are the barriers to adoption? J Am Acad Dermatol. 2020;83(1):299–307. CrossRef | PubMed
- 22. Australian Radiation Protection and Nuclear Safety Agency. Ultraviolet radiation index. Melbourne: Australian Government; 2021 [cited 2021 Dec 13]. Available from: www.arpansa.gov.au/our-services/monitoring/ultraviolet-radiation-monitoring/ultraviolet-radiation-index