Abstract
Health promotion in workplace settings has been prioritised to reduce chronic disease risk factors, both in Australia and internationally. This paper describes the design of a health risk assessment tool, the Brief Health Check (BHC). The BHC is one of two components of Get Healthy at Work, a state government-funded health promotion program for New South Wales workplaces.
Policy imperatives required scaled-up delivery in the absence of a full pre-implementation summative evaluation. Translational formative evaluation was adapted to design an evidence based health risk assessment tool, a process for referring workers to healthy lifestyle programs, and a process for general practitioners to help workers mitigate their risk of chronic disease, independently of the workplace.
The tool had good feasibility and acceptance, but barriers included business organisational issues (including the time taken to facilitate the health checks) and some scepticism among workers about the motivation of businesses and the absence of measurements other than waist circumference. A cluster nonrandomised trial showed no benefit of a modest incentive for participation. A significant proportion of workers were identified as being at risk of chronic disease, and many received an appropriate referral to an evidence based program. More work to improve uptake of referrals will increase the public health impact of the BHC.
Full text
Background
The World Health Organization (WHO) has prioritised the workplace as a key setting for health promotion in the 21st century.1 In Australia, the former National Partnership Agreement on Preventive Health funded jurisdictions to implement workplace health programs to reduce chronic disease risk factors among workers aged 35–55.2 In New South Wales (NSW), the workplace is a central component of the Healthy Eating and Active Living Strategy.3
The workplace presents unique challenges for health promotion programs. To ensure delivery at scale, programs should meet the requirement of workplaces for simplicity and ease of implementation, but be delivered at an intensity sufficient to replicate the effectiveness seen in research studies. The requirement of workers and worker organisations for confidentiality and autonomy must be included during implementation.4,5
This paper describes the design of the Brief Health Check (BHC), one of two components of the program, Get Healthy at Work (GHaW). The BHC is a health risk assessment (HRA) tool, which aims to establish an individual worker’s risk of diabetes and cardiovascular disease (CVD), improve understanding of modifiable risk factors, increase participation in healthy lifestyle programs to reduce this risk, and refer high-risk workers to a general practitioner (GP) for medical assessment. A Workplace Health Program (WHP) is designed to create health promoting structures and processes in the workplace. Overall, GHaW aims to reduce risk factors for type 2 diabetes and CVD. The targeted risk factors are overweight and obesity, diet and nutrition, physical activity and smoking (see www.gethealthyatwork.com.au for more information).
Approach
Evidence based decision making and program design are well established in population health.6 Frameworks for translating research to practice typically focus on replicating programs with good evidence to determine their effectiveness in other settings and populations.7 A well-known Australian example is the Sydney Diabetes Prevention Program, where lifestyle programs known to be effective were used to reduce risk factors of patients attending GPs.8 For the BHC, there was no single evidence based intervention available, and it was not feasible to undertake full pre-implementation design and research.
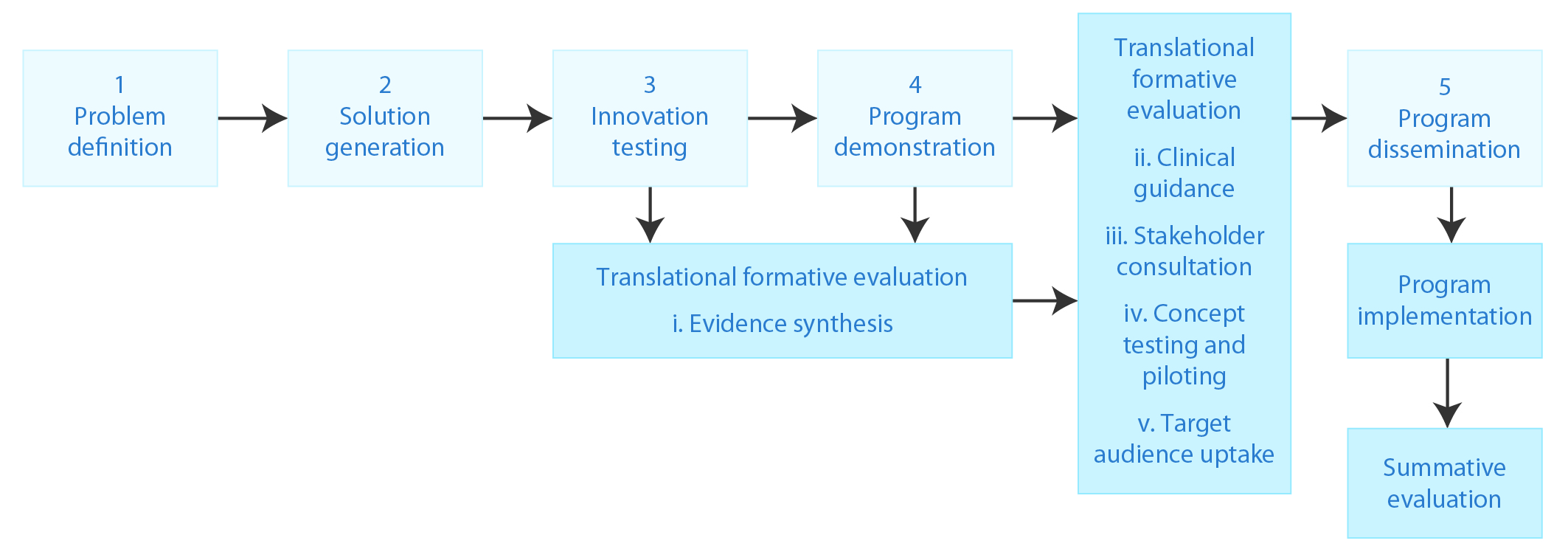
To ensure an evidence based health risk assessment, and to address challenges inherent in workplace health promotion, we used translational formative evaluation (TFE), described by O’Hara and colleagues9, which is an adaptation of Nutbeam and Bauman’s rocket model.10 TFE allows integration of evidence from a range of sources with program planning processes that consider context, stakeholder views and target population responses to proposed program components. We also pilot tested the proposed HRA to assess feasibility and participation. Thus, for BHC development, TFE had five components:
- Evidence synthesis
- Clinical guidance
- Stakeholder consultation
- Concept testing and piloting
- Evaluation of target population participation.
Figure 1 shows each component (shaded) with the standard components of the rocket model (not shaded). In the following sections, the method and findings for each component are described.
Figure 1. The translational formative evaluation model applied to the development of the Get Healthy at Work Brief Health Check
Evidence synthesis
For the evidence synthesis step, we reviewed the HRA research for improvements in risk factors (e.g. smoking cessation), improvements in combined risk factors scores, proposed BHC components and programs for referral of at-risk participants.
For the targeted health outcomes, systematic reviews showed a strong association of HRA with smoking cessation, and evidence from individual studies for their effectiveness to control overweight and obesity.11 However, the effectiveness of HRAs for improving physical activity and fruit and vegetable consumption was equivocal.12 For risk factor scores, there is a moderate effect of HRA (with additional workplace interventions) on score reduction.11,12
With a desire to ensure suitability for the Australian context, we determined the usefulness of risk assessment tools for diabetes and CVD. The Australian type 2 diabetes risk assessment tool (AUSDRISK)13 predicts a 5-year risk of diabetes using easily assessed risk factors, and includes ethnic- and sex-specific cut-off points for waist circumference. Risk assessment for CVD was developed with advice from the GHaW Clinical Advisory Panel (see ‘Clinical guidance’).
Finally, we determined the potential effectiveness of available programs for referral of participants with increased risk of diabetes or CVD, and smokers. The Get Healthy Information & Coaching Service (GHS) demonstrates validated reductions of 5 cm from waist circumference and 4 kg from weight, and significant increases in fruit and vegetable consumption and physical activity.14 It was deemed appropriate for workers with elevated risk of diabetes and CVD, and it has a diabetes-prevention module. Similar programs have been shown to be effective for risk reduction among high-risk individuals.15 For smokers, NSW Quitline16 is based on telephone counselling models known to support people to quit smoking.17
Clinical guidance
A Clinical Advisory Panel gave guidance on clinical aspects of the BHC, including appropriate advice, follow-up and participant duty of care.18 For CVD risk, waist circumference – using WHO cut-off points endorsed by the National Health and Medical Research Council – was considered an appropriate method of risk assessment.19 For workers at high risk of either CVD or diabetes, a GP referral was deemed necessary in addition to program referral. The panel also advised that alcohol consumption should be assessed and advised on, because of the strong association between alcohol consumption and chronic disease.
The AUSDRISK is not validated for the general population younger than 40 years and Aboriginal people aged less than 18 years. The panel recommended that advice for these workers should be on the basis of responses to specific AUSDRISK tool questions only.18
Stakeholder consultation
The primary method of stakeholder consultation was a key stakeholder forum with representatives from industry, government, nongovernment and professional organisations. The proposed key elements of the service were presented, followed by group work sessions to identify challenges and opportunities. This discussion generated a rich interpretation of how the BHC could function and be perceived by workers. The program overall was received positively. For the BHC, the opportunity to refer workers to other NSW Health services and GPs was viewed favourably, because it could extend the benefits of existing NSW program referrals to potentially thousands of people. Motivating worker participation in the BHC was considered challenging, however. Furthermore, there was concern, addressed subsequently by the program Clinical Advisory Panel, that workers needed clarity that the BHC was not a replacement for consultation with a medical practitioner.
Consultation with stakeholders representing workers identified concerns about worker confidentiality and autonomy, and the potential for the results to be used to discriminate against individual workers; these concerns have also been identified in the literature.4,5 A number of elements were embedded into the design of the program to ensure autonomy and privacy. Individual BHC results would be given only to that individual, and de-identified summary reports of key health measures would be provided to a business only when a minimum of 50 BHCs were undertaken. Finally, off-site referral to healthy lifestyle programs and GPs supports workers to manage lifestyle risk factors independently of their workplace.
Concept testing and piloting
The design and finalisation of the BHC took place in three phases at worksites with decreasing commitment to workplace health. In phase 1, 53 draft BHCs were conducted face to face at an office of our partner organisation, SafeWork NSW, to test its responsiveness to the concept of a BHC and its proposed components. Subsequently, pilots in two worksites of businesses with a total of 310 employees, with management interviews and worker focus groups, were conducted approximately 1 week after completion of the BHCs to allow time for reflection while minimising recall bias. Of the available (i.e. rostered on) workforce, 75 (more than 40%) participated in the BHC and, of those, 53 (70%) completed the evaluation survey.
The results demonstrated acceptability, simplicity and ease of delivery within a 15-minute time frame, but issues arose in several areas. Promotion of the BHC required significant time and organisational issues, such as shift arrangements, which prevented wider participation. Some workers demonstrated scepticism about the motivation of businesses, the absence of blood pressure measurement and blood tests, and data confidentiality. There was also a preference for visiting their own doctor (particularly among women) and a lack of perceived need for an HRA.
Target population participation
Participants in workplace health promotion research are, for the most part, self-selecting, which reduces the promise of reach and effectiveness in practice.11 There is also some evidence that participation may be poorer in larger businesses.12
To explore participation further, the finalised BHC was piloted at nine businesses within transport and manufacturing industries at 16 worksites with 1719 workers (Table 1). In total, 26.9% of workers participated in the BHC, with a highly variable range of 7–100% of workers. The results confirmed an association between business size and BHC participation, with larger businesses having lower participation.
Table 1. Brief Health Check participation in nine pilot businesses
| Location | Business type | Worksites | Workers | No. of participants (%) |
| Metro | Transport | 4 | 850 | 154 (18.1) |
| Metro | Manufacturing | 1 | 90 | 52 (57.8) |
| Metro | Manufacturing | 1 | 96 | 7 (7.3) |
| Metro | Transport | 2 | 200 | 48 (24.0) |
| Regional | Transport | 1 | 80 | 53 (66.3) |
| Regional | Manufacturing | 4 | 359 | 121 (33.7) |
| Regional | Manufacturing | 1 | 30 | 15 (50.0) |
| Regional | Transport | 1 | 10 | 10 (100.0) |
| Regional | Transport | 1 | 4 | 2 (50.0) |
| Total | 16 | 1719 | 462 (26.9) |
Subsequently, GHaW was implemented in another business (in the finance industry) to determine the impact of an incentive on participation. The use of incentives to achieve desirable social outcomes has been previously demonstrated20, and it was thought that some businesses may wish to establish an incentive scheme to encourage participation. We also tested two engagement strategies. The BHC is designed so that the individual worker makes their own appointment. We hypothesised that workers may be more likely to attend the BHC appointment if the appointment was scheduled (with permission) by their employer.
The study population was call-centre operators. This is a low-control and high-demand job, which is broadly representative of occupational groups known to have relatively poor health in a number of industries targeted by GHaW, such as manufacturing.21
The South Western Sydney Local Health District Human Research Ethics Committee approved a cluster nonrandomised trial with three arms (make own appointment, scheduled appointment and scheduled appointment with an incentive). On average, BHC participation was 29%, irrespective of appointment type, with no additional effect of a modest incentive (Table 2).
Table 2. Participation in the Brief Health Check for three methods of engagement
| Method | Workers | No. of participants (%) |
| Make own appointment | 80 | 21 (26.3) |
| Scheduled appointment | 226 | 67 (29.6) |
| Scheduled appointment with incentive | 133 | 40 (30.1) |
| Total | 439 | 128 (29.2) |
We also tracked acceptance of referral to the GHS and Quitline. Of 128 workers participating in the BHC, 103 (80%) had increased or high risk of heart disease and/or diabetes. Of these, only 45 (35%) were referred to the GHS, 32 of whom agreed to a referral being faxed to the service. Of the 18 who were contacted, 14 agreed to have coaching and 3 agreed to receive information only. At the 6-month follow-up with the GHS, 5 participants had continued in the coaching service, representing 5/18 benefiting from the GHS, but only 5/103 of those initially identified at risk.
Table 3. Referrals to NSW Quitline and Get Healthy Information & Coaching Service
| Service | At risk (%) | Recommended (%) | Referral accepted(%) | Enrolled(%) | Continuing(%) |
| Quitline | 34 (27) | 28 (22) | 13 (10) | 8 (6) | 1 (–) |
| GHS | 103 (80) | 45 (35) | 32 (25) | 14 (11)a | 5 (4.8) |
a An additional 3 participants received information only, an option offered by Get Healthy Information & Coaching Service (GHS).
Note: Percentages are the percentage of all Brief Health Check participants.
Of the BHC participants, 27% were current smokers or smoked within the previous year. Of these, 28 (22%) were offered a referral to Quitline, and 13 agreed to have the referral faxed to the service. At the 6-month follow-up, only 1 participant was continuing with Quitline.
Discussion
The BHC was developed within a context of significant government support for workplace health programs. An adapted TFE approach9 with five components provided a useful framework for the design of an evidence based HRA, and an understanding of potential reach and barriers to, and enablers of, participation. The evidence review indicated that HRA is associated with improvements in some of the health behaviours targeted by the BHC. There is also evidence that risk factor scores may be reduced when used within the context of workplace health programs, suggesting that the program overall may have the capacity to reduce diabetes risk as measured by the AUSDRISK tool.12,13 Although associations between HRA and physical activity and fruit and vegetable consumption have not been established at this stage, we can be confident that referrals to the GHS improve these risk factors.
Worker autonomy and confidentiality were built into the protocol for BHCs, and stakeholder consultation revealed a number of issues, which were dealt with in the development of the program. Pilot sites, and a trial of worker engagement strategies and incentivisation showed acceptable worker participation of around 30%. Optimising worker participation requires ongoing consideration and resolution, and is affected by worker and business barriers (particularly in larger workforces), and acceptance of referrals and completion of programs. This will be a key challenge to the success of the BHC in contributing to reaching population health goals.
Competing interests
None declared
Author contributions
BL drafted and finalised the manuscript. SK, EM and CR reviewed and contributed to the manuscript. All authors were engaged in the process of development of the Brief Health Check.
Copyright:

© 2016 Lloyd et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation (WHO technical report series 894). Geneva: WHO; 2000 [cited 2016 Aug 10]. Available from: www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/
- 2. Council of Australian Governments. National partnership agreement on preventive health. Canberra: Commonwealth of Australia; 2008. [cited 2016 Sep 14]. Available from: www.federalfinancialrelations.gov.au/content/npa/health/archive/national-overview.pdf
- 3. NSW Government. NSW healthy eating and active living strategy: preventing overweight and obesity in NSW 2013–2018. Sydney: NSW Ministry of Health; 2013 [cited 2016 Aug 10]. Available from: www.health.nsw.gov.au/heal/Publications/nsw-healthy-eating-strategy.pdf
- 4. Rothstein MA, Harrell HL. Health risk reduction programs in employer-sponsored health plans: part 2 – law and ethics. J Occup Environ Med. 2009;51(8):951–7. CrossRef | PubMed
- 5. van Berkel J, Meershoek A, Janssens R, Boot C, Proper KI, van der Beek AJ. Ethical considerations of worksite health promotion: an exploration of stakeholders’ views. BMC Public Health. 2014;14:458. CrossRef | PubMed
- 6. Brownson RC, Chriqui JF, Stamatakis KA. Understanding evidence-based public health policy. Am J Public Health. 2009;99(9):1576–83. CrossRef | PubMed
- 7. Rychetnik R, Bauman A, Laws L, King L, Rissel C, Nutbeam D, et al.. Translating research for evidence-based public health: key concepts and future directions. J Epidemiol Community Health. 2012;66:1187–92. CrossRef | PubMed
- 8. Vita P, Cardona-Morrell M, Bauman A, Singh M, Moore M, Pennock R, et al. Type 2 diabetes prevention in the community: 12-month outcomes from the Sydney Diabetes Prevention Program. Diabetes Res Clin Pr. 2015; 112:13–9. CrossRef | PubMed
- 9. O'Hara B, Phongsavan P, King L, Develin E, Milat A, Eggins D, et al. 'Translational formative evaluation': critical in up-scaling public health programmes. Health Promot Int, 2014;29(1):38–46. CrossRef | PubMed
- 10. Nutbeam D, Bauman A. Evaluation in nutshell: a practical guide to the evaluation of health promotion programs. Sydney: McGraw-Hill; 2006.
- 11. Bellew B, St George A, King L. Workplace screening programs for chronic disease prevention: an Evidence Check brokered by the Sax Institute for the NSW Ministry of Health. Sydney: The Sax Institute; 2012 [cited 2016 Aug 10]. Available from: www.saxinstitute.org.au/wp-content/uploads/04_Workplace-screening-programs-for-chronic-disease-preventi.pdf
- 12. Soler RE, Leeks KD, Razi S, Hopkins DP, Griffith M, Aten A, et al. A systematic review of selected interventions for worksite health promotion. The assessment of health risks with feedback. Am J Prev Med. 2010;38(2 Suppl):S237–62. CrossRef | PubMed
- 13. Chen L, Magliano DJ, Balkau B, Colagiuri S, Zimmet PZ, Tonkin AM, et al. AUSDRISK: an Australian type 2 diabetes risk assessment tool based on demographic, lifestyle and simple anthropometric measures. Med J Aust. 2010;192(4):197–202. PubMed
- 14. O’Hara BJ, Phongsavan P, McGill B, Maxwell M, Ahmed N, Raheb S, Bauman AE. The NSW Get Healthy Information and Coaching Service: the first five years. Sydney: NSW Ministry of Health; Prevention Research Collaboration, University of Sydney; 2014 [cited 2016 Aug 10]. Available from: www.gethealthynsw.com.au/assets/pdf/medicalprofessionals/resources/Get_Healthy_Service_Evaluation_Report_WEB_version.pdf
- 15. Tuomilehto J, Lindström J, Qiao Q. Strategies for the prevention of type 2 diabetes and cardiovascular disease. Eur Heart J Suppl. 2005;7(Suppl D):D18–D22. CrossRef
- 16. Grunseit AC, Ding D, Anderson C, Crosbie D, Dunlop S, Bauman A. A profile of callers to the New South Wales Quitline, Australia, 2008–2011. Nicotine Tob Res. 2015;17(5):617–21. CrossRef | PubMed
- 17. Stead LF, Hartmann-Boyce J, Perera R, Lancaster T. Telephone counselling for smoking cessation (review). Cochrane Database Syst Rev. 2006;(3):CD002850. CrossRef
- 18. NSW Ministry of Health. Clinical guidance for health practitioners conducting the Brief Health Check. Sydney: NSW Ministry of Health; 2015.
- 19. National Health and Medical Research Council. Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: NHMRC; 2013 [cited 2016 Aug 10]. Available from: www.nhmrc.gov.au/guidelines-publications/n57
- 20. Bornstein G, Gneezy U, Nagel R. The effect of intergroup competition on group coordination: an experimental study. Games and Economic Behavior. 2002;41(1):1–25. CrossRef
- 21. Karasek RA, Theorell T. Healthy work: stress, productivity and the reconstruction of working life. New York: Basic Books; 1990.