Abstract
Introduction: In Australia, adult immunisation coverage is primarily monitored via periodic telephone surveys that rely on self-reported immunisation status. All Australian residents are eligible for Medicare, so we examined the feasibility of using immunisation-specific Medicare Benefits Schedule (MBS) item numbers to monitor and estimate adult influenza immunisation coverage.
Methods: Baseline questionnaire data from 267 129 participants from the 45 and Up Study, a prospective cohort study, were linked to data containing information on individual MBS immunisation-specific items from 2006 to 2011. Temporal trends in recording of these items were examined. Self-reported influenza immunisation status obtained from a follow-up questionnaire from 27 036 participants was then compared with the MBS immunisation records.
Results: From 2006 to 2011, the pattern of MBS immunisation claims was consistent with self-reported influenza immunisation trends, with annual peaks occurring from March to May. There was fair agreement between MBS immunisation records and self-reported influenza immunisation: 48.8% (95% CI 47.1, 50.4) of participants who self-reported influenza immunisation had a matching MBS record, and 79.6% (95% CI 78.8, 80.4) who reported never having influenza immunisation had no matching MBS record. However, compared with self-reported influenza vaccination for people aged ≥65 years from the 2009 Adult Immunisation Telephone Survey (74.6%), the proportion of participants aged >65 years with an MBS immunisation record was low, with an annual median of 39.3% (range 28.3%–62.1%).
Conclusion: MBS immunisation item data are readily available and may be useful to monitor trends in adult influenza immunisation, but they are likely to substantially underestimate coverage. Other approaches, such as capture of general practitioner-delivered influenza vaccine doses or a whole-of-life immunisation register, are needed to comprehensively monitor and estimate adult immunisation coverage for influenza and other recommended adult vaccines.
Full text
Introduction
Adult influenza immunisation is an important public health intervention that significantly decreases morbidity and mortality, and associated economic costs, resulting from influenza infection.1,2 An important measure of vaccine program success is coverage. In Australia, childhood immunisation coverage to the age of 7 years can be monitored using the Australian Childhood Immunisation Register3 and the National HPV [human papillomavirus] Vaccination Program Register4, which measures adolescent and young adult HPV vaccine coverage. However, there is no national register to measure older adult immunisation. Therefore, national coverage is estimated primarily through self-reported immunisation status collected via periodic telephone surveys.5
For adults, the National Immunisation Program funds influenza immunisation for adults aged ≥65 years, adults aged <65 years who are at higher risk of influenza, and Aboriginal and Torres Strait Islander people aged ≥15 years.6 Measuring adult influenza immunisation coverage is important to enable the vaccination program to be properly evaluated and improvements to be made. For example, populations with lower coverage may be identified and targeted with more specific health promotion campaigns. Understanding coverage in adults is increasingly important as the Australian population ages7 and as more adult vaccines are approved (e.g. herpes zoster vaccine).
Use of administrative or electronic health records is a potential method by which adult immunisation coverage could be monitored. Electronic data extracted from Australian primary healthcare settings have been used to monitor immunisation coverage in adults, but these only cover selected populations.8,9 All Australian residents, and visitors from countries that have a ‘reciprocal healthcare agreement’, are eligible for Medicare, the national health insurance program.10 Two item numbers cover immunisation services provided by practice nurses. These were not designed to capture all immunisations, but we hypothesised that they might be a useful mechanism for monitoring adult influenza immunisation coverage and trends in Australia.
Methods
Study population
This study used data from the Sax Institute’s 45 and Up Study, a prospective cohort of 267 129 adults aged 45 years and older. The study recruitment methods have been described elsewhere.11 Briefly, New South Wales (NSW) residents aged 45 years and older were randomly sampled from the Medicare Australia enrolment database, with oversampling of those aged ≥80 years, and rural and remote residents, and invited to take part in the study. Between 2006 and 2009, participants completed a questionnaire and agreed to be contacted periodically to complete further surveys and also have their data linked to administrative health datasets, including the Medicare Benefits Schedule (MBS). In 2012, 41 413 participants were asked to complete a questionnaire with the questions, ‘Have you ever had the flu vaccine?’ and ‘If yes, when did you last have the flu vaccine (month and year)?’12 At the time of analysis, 27 036 participants had completed and returned this questionnaire.
Medicare Benefits Schedule
The MBS records data about claims made by patients for medical services that are reimbursable under Medicare. Reimbursable health services are identified with specific item numbers. Two immunisation-specific item numbers were listed in the MBS, and available between 2006 and 2011: 10993 (immunisation provided by a practice nurse) and 10988 (immunisation provided by an Aboriginal health worker).13 Both items terminated in 2012. These item numbers covered all practice-based immunisations and were not specific to influenza. They were introduced as part of the Practice Incentives Program and were only used by practices in the program. Immunisations not captured by these item numbers were those recorded by general practitioners as a ‘standard attendance’ item. The MBS does not record other influenza immunisations – for example, through workplace programs.
Linkage and analysis
Using a unique but anonymised personal identifier, all 45 and Up Study participants were linked to their corresponding MBS immunisation item numbers from 1 January 2006 to 31 December 2011. We first examined the frequency of MBS immunisation item numbers recorded for the entire cohort, according to the date of service provision. We then restricted analyses to those 27 036 participants for whom we had self-reported data on influenza immunisation status, and determined whether they had a linked MBS immunisation record. We calculated the percentages of people reporting an influenza immunisation who had at least one MBS record of immunisation, and those not reporting an influenza immunisation for whom there was no MBS record of immunisation.
Overall agreement was calculated using the number of people who self-reported having an influenza vaccination who had an MBS record for immunisation, combined with those not reporting an influenza immunisation for whom there was no MBS record of immunisation. The analysis was conducted in two different groups to ensure that findings were consistent and not due to assumptions made in the analysis regarding time frame. Comparisons were made for all participants, with participants who ever reported an influenza vaccination being linked to an MBS record, if available. The analysis was then restricted to 45 and Up Study participants who reported an influenza immunisation from 2006 to 2011 (inclusive), which corresponded to the period for which we had MBS immunisation item number records. This subset of participants was linked to an MBS record, if available.
Chi-square tests were used to test for significant differences in proportions.
Results
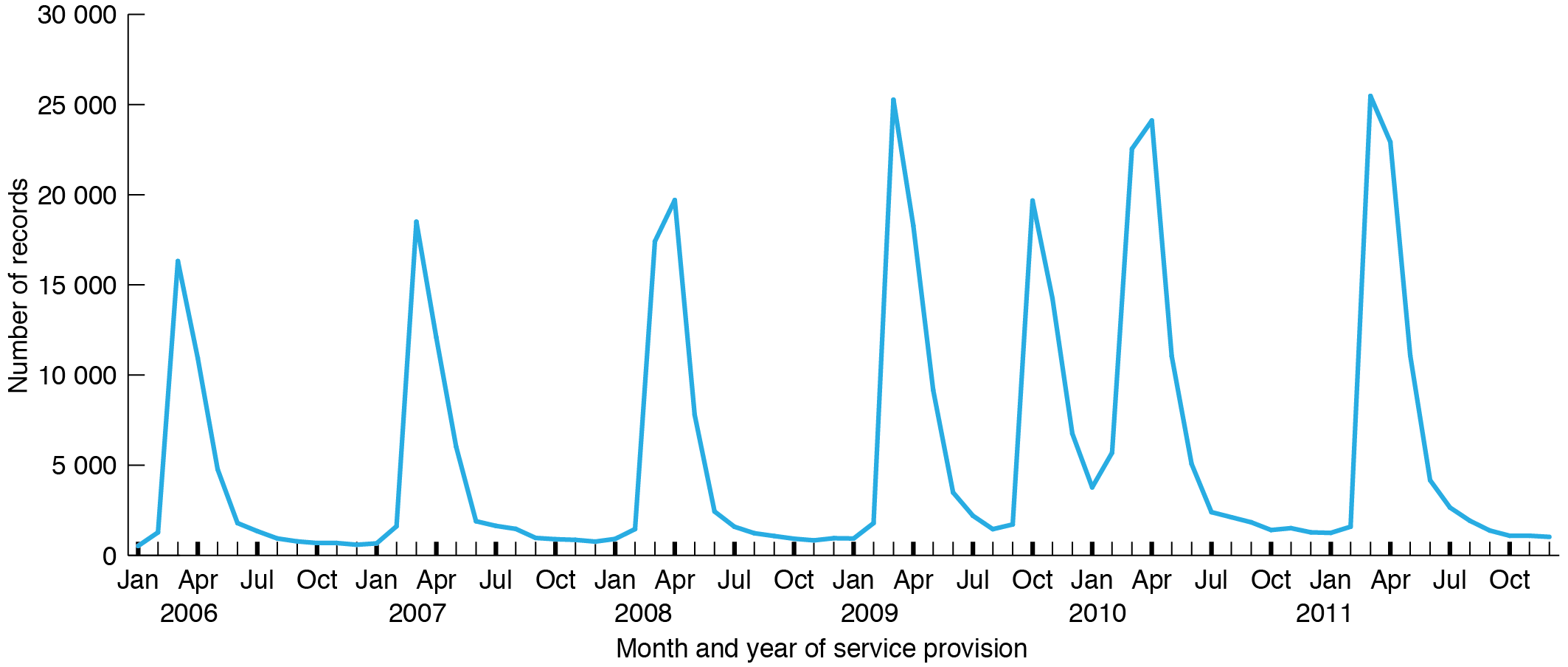
Of 267 129 participants in the 45 and Up Study, 37 908 (14.2%) were linked with one, and 84 791 (31.7%) with more than one, MBS immunisation record. Annually, the total number of immunisation item numbers recorded for the linked participants ranged from 40 660 to 104 998 (median 65 999), giving a median annual percentage of participants with at least one linked immunisation record of 24.7% (range 15.2–39.3%). For participants aged ≥65 years the equivalent numbers ranged from 29 235 to 64 190 (median 40 639), giving a median annual percentage of participants aged >65 years with at least one linked immunisation record of 39.3% (range 28.3%-62.1%). Figure 1 shows the trend over time in the frequency of use of MBS immunisation item numbers among the study participants. In each year, the peak in MBS immunisation records occurred between March and May. There was also an additional peak in October 2009. This pattern was similar in both <65 years and ≥65 years age groups.
Figure 1. Number of MBS immunisation records linking to 45 and Up Study participants by month and year of service provision, January 2006 to December 2011 (click to enlarge)
After restricting analyses to the 27 036 study participants who self-reported influenza immunisation, 4080 (15.1%) participants linked with only one, and 8588 (31.8%) with more than one, MBS immunisation record. Of those who reported ever having an influenza immunisation, 58.4% (95% CI 57.7, 59.1) had at least one MBS immunisation record. Of those never reporting influenza immunisation, 79.8% (95% CI 79.0, 80.7) did not have an MBS immunisation record (Table 1).
Table 1. Comparison of participants who self-reported ever having an influenza immunisation with MBS immunisation records, 2006–2011
| MBS immunisation record | |||
| Self-report | Ever | Never | Total |
| Ever (%) | 11 018 (58.4) | 7 834 (41.6) | 18 852 (100.0) |
| Never (%) | 1 650 (20.2) | 6 534 (79.8) | 8 184 (100.0) |
| 27 036 | |||
MBS = Medicare Benefits Schedule
When we restricted the analyses further to cohort members who specifically reported an influenza immunisation at least once between 2006 and 2011, and those never reporting an influenza immunisation (to correspond to the same time period for which we had MBS records), there were 12 733 people remaining. Of 3786 people reporting having an influenza vaccination in this period, 48.8% (95% CI 47.2, 50.4) had an MBS record. Of those never having reported an influenza vaccination (n = 8947), 79.6% (95% CI 78.8, 80.4) had no MBS record. Overall agreement between the two sources was 70.4% (8969/12 733; 95% CI 69.6, 71.2) (Table 2).
Table 2. Comparison of participants who self-reported an influenza immunisation in 2006–2011 with MBS records, 2006−2011
| MBS immunisation record | |||
| Self-report | Ever | Never | Total |
| Ever (%) | 1 846 (48.8) | 1 940 (51.2) | 3 786 (100.0) |
| Never (%) | 1 824 (20.4) | 7 123 (79.6) | 8 947 (100.0) |
| 12 733 | |||
MBS = Medicare Benefits Schedule
When we stratified results by age, overall agreement was similar, at 70% for those aged <65 years and 71% for those aged ≥65 years (see Table 3). However, a lower proportion of those <65 years who self-reported an influenza immunisation had a corresponding MBS record (43%, compared with 57% for ≥65 years, p < 0.01). There was, however, no significant difference in this proportion when results were stratified by sex (48.6% in men, 48.9% in women; p = 0.8).
Table 3. Comparison of participants who self-reported an influenza immunisation with MBS records by age and sex, 2006−2011
| MBS record | |||||
| Self-report | Ever (%) | Never (%) | Total (%) | ||
| By age group | <65 yrs | Ever | 1 000 (43.3) | 1 309 (56.7) | 2 309 (100.0) |
| Never | 1 198 (19.9) | 4 836 (80.1) | 6 034 (100.0) | ||
| ≥65 yrs | Ever | 846 (57.3) | 631 (42.7) | 1 477 (100.0) | |
| Never | 626 (21.5) | 2 287 (78.5) | 2 913 (100.0) | ||
| By sex | Men | Ever | 767 (48.6) | 812 (51.4) | 1 579 (100.0) |
| Never | 714 (18.4) | 3 158 (81.6) | 3 872 (100.0) | ||
| Women | Ever | 1 079 (48.9) | 1 128 (51.1) | 2 207 (100.0) | |
| Never | 1 110 (21.9) | 3 965 (78.1) | 5 075 (100.0) | ||
MBS = Medicare Benefits Schedule
Discussion
In this cohort of older adults, we found a seasonal trend in the frequency of use of MBS immunisation item numbers, with the majority of immunisations occurring in the months before winter, consistent with seasonal influenza immunisation. The additional peak in MBS immunisation records observed in October 2009 coincided with the availability in Australia of the H1N1-specific vaccine to combat the 2009 swine influenza epidemic.14 This correlation suggests that the MBS immunisation item numbers represent a large proportion of influenza immunisations.
The trends were consistent with other data sources1, but the annual total number of records was lower than might be expected for influenza immunisation in this age group. The 2009 Adult Vaccination Survey found that 74.6% of those aged ≥65 years reported influenza vaccination that year1, whereas we found a proportion ranging from 28.3% to 62.1% of study participants aged ≥65 years with an MBS immunisation item number recorded in each year of observation. The higher end of this range occurred in 2009, when H1N1 influenza vaccination was introduced. The apparent underestimate in coverage in our analysis was consistent with the comparison of individual self-reports of influenza immunisation with MBS data. There was good agreement for participants who self-reported never having an influenza immunisation, with 80% having no corresponding MBS record, but, for those self-reporting influenza immunisation, less than half had a matching record in the MBS dataset. The level of agreement between those self-reporting an influenza immunisation and the MBS record was slightly better in adults aged ≥65 years than in those aged <65 years, possibly because people aged <65 years may access immunisation services in non–primary care settings, such as the workplace. Such programs are unlikely to be reimbursable through Medicare.
To the best of our knowledge, no other studies have examined the use of MBS data as a method to monitor trends and estimate adult influenza immunisation coverage in Australia. The use of data from primary care to monitor adult immunisation has been previously explored in several different settings in Australia. For example, extraction of data from general practices in Western Australia has been shown to be a feasible method for estimating influenza immunisation coverage. However, this method of measurement requires specific data extraction software to be installed at general practices, so may not be adaptable to a national scale. Two Australian jurisdictions, the Northern Territory and Queensland, have state-based immunisation registers that collect information on all government-funded adult immunisations. Both registers collect immunisation data from all primary care settings and hospitals. They require practitioners to report immunisations via a paper report form and manual data entry, making them labour intensive.
A number of factors may have contributed to the lack of agreement between the two data sources regarding influenza immunisation. The MBS immunisation item numbers were designed to capture practice nurse–administered immunisation only and are not specific for influenza. Therefore, although the seasonal trends in the MBS immunisation data suggest that the majority of records are related to influenza vaccine, the item numbers could also have been recorded for any other vaccinations provided by practice nurses in the community setting, such as pneumococcal, travel or healthcare worker vaccines. MBS immunisation records do not record influenza immunisations received through workplace programs or other settings, such as in public hospitals. Furthermore, not all immunisations in general practice necessarily resulted in an immunisation-specific MBS item number being recorded. For example, the immunisation may be given as part of a broader patient consultation, and the practitioner may not make a specific MBS claim for it, or could use an attendance item number. Immunisations given by other providers not included in the Practice Incentives Program would also not be captured.
Previous studies have suggested that self-reported influenza immunisation status is highly sensitive15,16; however, the self-reported data from the 45 and Up Study may be affected by recall bias, particularly in relation to the timing of the vaccination, and this may also have affected the level of agreement. Limitations associated with each dataset highlight that there is currently no gold standard to monitor adult vaccination status and coverage in Australia, as the Australian Childhood Immunisation Register does for childhood vaccinations.
Conclusion
We investigated the use of routinely collected data to inform adult influenza immunisation coverage. Our findings suggest that previous MBS immunisation-specific items numbers (10993 and 10988) may have been useful to monitor trends or for surveillance of influenza immunisation in adults; however, they were not sufficiently precise and underestimated total influenza immunisation coverage. Our results highlight the difficulty in determining adult immunisation coverage in Australia using current routinely collected data. As part of the 2015 federal Budget, the government announced plans to introduce a whole-of-life immunisation register17 to record all adult vaccines provided under the National Immunisation Program. The challenge will now be to efficiently collect accurate and comprehensive data for such an adult register.
Acknowledgements
This research was completed using data collected through the 45 and Up Study, which is managed by the Sax Institute in collaboration with major partner Cancer Council NSW and partners: the National Heart Foundation of Australia (NSW Division), the NSW Ministry of Health, beyondblue, the NSW Department of Family & Community Services – Carers, Ageing and Disability Inclusion, and the Australian Red Cross Blood Service. We thank the many thousands of people participating in the 45 and Up Study. This study was funded by a National Health and Medical Research Council (NHMRC) project grant (APP1048180). AD is a recipient of an NHMRC PhD scholarship. EB, JK and BL hold NHMRC Fellowships.
Copyright:

© 2015 Dyda et al. This article is licensed under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Colgan S, Tay-Teo K, Shih S, Carter R. Influenza vaccination for ‘at risk’ Australian adults aged between 18 to 64. Part 2 of the cost-of-illness study of current practice and cost analysis of extending vaccination to all ‘at risk’ Australian adults. Canberra: National Institute of Clinical Studies; 2006 [cited 2015 Aug 19]. Available from: dro.deakin.edu.au/eserv/DU:30010506/carter-influenzavaccinationatriskpart2-2006.pdf
- 2. Newall AT, Scuffham PA. Influenza-related disease: the cost to the Australian healthcare system. Vaccine. 2008;52(26):6818–23. CrossRef | PubMed
- 3. Department of Health. Australian childhood immunisation register. Canberra: Australian Government; 2015 [cited 2015 Aug 19]. Available from: www.humanservices.gov.au/customer/services/medicare/australian-childhood-immunisation-register
- 4. Department of Health and Ageing. National HPV Vaccination Program Register. Canberra: Australian Government; 2015 [cited 2015 Aug 15]. Available from: www.hpvregister.org.au
- 5. Australian Institute of Health and Welfare. 2009 adult vaccination survey. Summary results. Canberra: Australian Institute of Health and Welfare; 2011 [cited 2015 Aug 19]. Available from: www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737418286
- 6. Department of Health. Immunise Australia program. Canberra: Australian Government; 2015 [cited 2015 Aug 19]. Available from: www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/immunise-influenza
- 7. Australian Bureau of Statistics. Population projections Australia 2006 to 2101. Canberra: Australian Bureau of Statistics; 2008 [cited 2015 Aug 19]. Available from: www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3222.02006%20to%202101?OpenDocument
- 8. Hanna JN, Young DM, Brookes DL, Dostie BG, Murphy DM. The initial coverage and impact of the pneumococcal and influenza vaccination program for at-risk Indigenous adults in Far North Queensland. Aust N Z J Public Health. 2001;25(6):543−6. CrossRef | PubMed
- 9. Hanna JN, Morgan AK, McCulloch BG. Uptake of influenza vaccine among Aboriginal and Torres Strait Islander adults in north Queensland, 2003. Commun Dis Intel. 2004:28(1):80−2.
- 10. Department of Human Services. Reciprocal health care agreements. Canberra: Australian Government; 2014 [cited 2015 Aug 19]. Available from: www.humanservices.gov.au/customer/services/medicare/reciprocal-health-care-agreements
- 11. Banks E, Redman S, Jorm L, Armstrong B, Bauman A, Beard J et al. Cohort profile: the 45 and up study. Int J Epidemiol. 2007;37(5):941−7. CrossRef
- 12. Sax Institute. 45 and Up Study questionnaires. Sydney: Sax Institute; [cited 2015 Aug 19]. Available from: www.saxinstitute.org.au/our-work/45-up-study/questionnaires
- 13. Department of Health. Medicare Australia. Canberra: Australian Government; [cited 2015 Jan 28]. Available from: www.medicareaustralia.gov.au
- 14. Department of Health and Ageing. Review of Australia’s health sector response to pandemic (H1N1) 2009: lessons identified. Canberra: Commonwealth of Australia; 2011 [cited 2015 Aug 19]. Available from: www.health.gov.au/internet/publications/publishing.nsf/Content/review-2011-l/$File/lessons%20identified-oct11.pdf
- 15. Mac Donald R, Baken L, Nelson A, Nichol KL. Validation of self-report of influenza and pneumococcal vaccination status in elderly outpatients. Am J Prev Med. 1999;16930:173−7. CrossRef | PubMed
- 16. Andrews RM. Assessment of vaccine coverage following the introduction of a publicly funded pneumococcal vaccine program for the elderly in Victoria, Australia. Vaccine. 2005;23(21):2756−61. CrossRef | PubMed
- 17. Australian Government. Budget 2015. Part 2: expense measures (continued). Canberra: Australian Government; 2015 [cited 2015 Aug 19]. Available from: www.budget.gov.au/2015-16/content/bp2/html/bp2_expense-14.htm