Abstract
Objectives: To report on efforts to engage culturally and linguistically diverse (CALD) communities to provide an effective and appropriate public health response to coronavirus disease 2019 (COVID-19), and to report how a tailored, interagency response addressing specific community needs was rapidly rolled out in a pandemic setting.
Type of program or service: A novel, rapid, interagency public health campaign led by NSW Health and Sydney Local Health District (SLHD) was established in response to a local outbreak of COVID-19 in the multicultural suburb of Lakemba, in Sydney’s south west, in October 2020. The public education and testing campaign was run over 2 weeks and involved in-language development of COVID-19 resources, establishment of a local pop-up testing clinic, ‘COVID Safe’ inspections of local businesses, engagement with local community leaders and distribution of written and verbal in-language education by cultural support workers.
Methods: We describe the campaign impact in engaging CALD communities in a pandemic setting, including the impact on COVID-19 testing rates, identification of close contacts and engagement with local businesses, as well as learnings from a multi-agency debrief at the conclusion of the campaign.
Results: There was an 87% increase in COVID-19 testing in the local area during the campaign. Despite 890 close contacts being identified during the outbreak, only 17 cases of COVID-19 were identified. Regulators visited 127 local businesses to provide ‘COVID Safe’ education and advice. SLHD cultural support personnel worked with the community to provide verbal and written in-language resources and education. Community and religious leaders were engaged to act as ‘COVID Safe’ champions.
Lessons Learnt: A key to the success of the Lakemba campaign was the rapid, multi-agency collaboration between NSW Health, SLHD and regulators. An important lesson from the COVID-19 pandemic has been the importance of providing a flexible, tailored public health response that reacts to the target community’s needs. This is even more important in our CALD communities, where mainstream health messages are insufficient. The Lakemba campaign is an example of how such a response can be undertaken rapidly while maintaining the key principles of community partnership, engagement and equity.
Full text
Background
During the pre-vaccine phase of the coronavirus disease 2019 (COVID-19) pandemic, the Australian response to eliminate and suppress COVID-19 was among the most successful internationally. New South Wales (NSW), the most populous state in Australia, demonstrated effective public health pandemic management1,2 due to long-term investment in public health and a well-resourced and integrated system. A decentralised structure of local health districts with embedded public health units enabled a timely, integrated and community-focused COVID-19 response.2 Community-level knowledge at the local health district level, paired with leadership and support provided through the Public Health Response Branch of the NSW Ministry of Health, allowed for effective, localised public health campaigns to suppress and control COVID-19 incursions and outbreaks.2,3
As such, NSW was uniquely positioned to mitigate the differential impacts of COVID-19 in marginalised and culturally and linguistically diverse (CALD) communities.4 Recent Australian participatory research has highlighted that successful engagement with CALD communities during the COVID-19 response requires partnerships with CALD leaders and communities and tailored messages based on community values.5 This paper describes a rapid, interagency public health campaign led by NSW Health and Sydney Local Health District (SLHD) in response to a local outbreak of COVID-19 in a CALD community in Lakemba, a suburb in south west Sydney.
In October 2020, NSW had very low rates of COVID-19 community transmission.6 Public health measures at that time included the closure of international (and some state) borders and mandatory hotel quarantine for all arrivals into the state. Mandatory isolation of COVID-19 cases and strict contact tracing were in effect. The previous public lockdown of March 2020 had been lifted, although capacity limits were in place at most venues and businesses were allowed to open with the requirement of a COVID-19 Safety Plan. Mandatory QR code check-ins were not yet in effect. There had been only one locally-acquired case in the state in the week preceding the first case in the Lakemba cluster.6 In the preceding month, a total of 49 locally-acquired cases had been identified, of which 94% were linked to known clusters or cases.6
On 10 October 2020, SLHD Public Health Unit (PHU) was notified of a confirmed case of COVID-19 in a community member who had attended a number of healthcare settings in the Lakemba area. Lakemba is a multicultural suburb in the south west of SLHD, in which 84.1% of the community identify both parents as being born overseas. The suburb includes large Bangladeshi (12.9%), Lebanese (7.7%), Indian (6.6%) and Pakistani (6%) populations.7 As a result of rapid contact tracing of the initial case, two healthcare workers from a Lakemba medical centre were identified as close contacts and tested positive for COVID-19 on 11 October. Over the following 2-week period, 17 confirmed cases of COVID-19 were linked to this cluster, with 890 close contacts identified through extensive contact tracing undertaken by SLHD PHU and NSW Health’s Close Contact Tracing Team.
Due to the large number of close contacts identified, NSW Health and SLHD PHU assessed the risk of community transmission as high. The sociodemographic profile of the Lakemba area meant that the population at risk included some of the most emerging, marginalised and vulnerable CALD communities in SLHD. These vulnerabilities are based on various factors, including recency of arrival, poor English language proficiency, refugee or asylum seeker status, household overcrowding, Medicare ineligibility and precarious work conditions. Such factors make it much harder for these communities to be reached through mainstream messaging on COVID risk factors and prevention strategies.5,8-10
A rapid, community-focused, interagency education campaign was developed, drawing on networks already established through the NSW Health ‘COVID Safe’ education and compliance program and drawing on the local community networks and knowledge of the SLHD PHU and Diversity Hub. The campaign ran from 12–25 October 2020 and aimed to minimise ongoing transmission by promoting ‘COVID Safe’ behaviours in the local community. This was the first time that a multi-agency response of its kind was undertaken by SLHD and the agencies involved.
This paper reports on how the campaign was rapidly rolled out and addresses the importance of engaging CALD communities effectively and appropriately in a pandemic setting.
An ethics application was not required for this study in accordance with the NSW Health Quality Improvement and Ethical Review policy requirements (Quality Improvement and Ethical Review GL2007_20).
Public health campaign objectives
The three main objectives of the program were:
- To raise awareness, in a culturally competent manner, of an elevated COVID-19 risk associated with the local cluster
- To establish a local in-language pop-up COVID-19 testing clinic and provide community information on various testing options
- To support local businesses to comply with COVID-19 safety requirements.
Campaign activities
Raising community awareness
SLHD undertook a broad-based engagement and information strategy that included the activities described below.
1. Community engagement via cultural support staff from the SLHD Diversity Programs and Strategy Hub (Diversity Hub).
The Diversity Hub is a unique team that uses content expertise and local community connections to support the district to be responsive and adaptive to working with priority CALD populations on various health issues. The cultural support staff undertook a range of activities, including:
- Facilitating in-language development of NSW Health resources into the major community languages of the Lakemba area (Arabic, Bangla, Chinese, Korean, Rohinga and Greek). This process involved a group of native speakers (two writers and two editors) working together to create the resource using a technically approved plain-English version as the base. The in-language version was reviewed by an independent community member from each language group for readability and appropriateness.
- Face-to-face in-language outreach with local businesses, venues and pre-existing community partners about the COVID-19 cluster, encouraging vigilance for symptoms and promotion of the local pop-up testing clinic.
- Preparation and distribution of in-language media releases and promotion of the pop-up testing clinic through various social media channels, local in-language print media and local in-language community radio.
2. Engagement of community religious leaders as ‘COVID Safe’ champions.
The SLHD PHU staff set up meetings with prominent religious leaders from the Lakemba area. The purpose of this engagement was to build rapport and share information with community leaders to promote COVID-Safe messages to congregations and community groups. No data was collected on the outcomes of these meetings.
Pop-up clinic and testing information
SLHD was also responsible for establishing a local pop-up COVID-19 testing clinic staffed specifically with cultural support workers, who provided a culturally safe space and assisted community members in translating health information. This was a walk-in clinic (no appointment required) situated in the Lakemba Uniting Church carpark. Data on test numbers was collected through the NSW COVID-19 statewide online register. No demographic data was available for analysis.
Supporting local businesses
NSW Health was responsible for rapidly engaging the relevant regulators and agencies and coordinating a brief cross-agency education and compliance campaign in the local business community in Lakemba. Agencies included SafeWork NSW, NSW Food Authority, NSW Department of Primary Industries, Liquor and Gaming NSW, NSW Fair Trading and NSW Department of Customer Service. The City of Canterbury Bankstown local council and NSW Police were consulted. Activities included:
- Inspections of businesses by regulators, primarily focusing on education and awareness
- A multi-agency debrief at the conclusion of the campaign.
The inspections aimed to ensure businesses understood their obligations under the Public Health (COVID-19 Restrictions on Gathering and Movement) Order (No 3) 2020 and to provide education and information to businesses to improve compliance. Such obligations included businesses complying with capacity restrictions and having a current COVID-19 safety plan, strategies for managing staff illness, appropriate hand hygiene practices for staff/customers and adequate record keeping. Inspectors recommended penalty infringement notices for businesses that were non-compliant with the majority of obligations under the Public Health Act. Businesses that demonstrated serious non-compliance with the Public Health Order were referred to NSW Health or NSW Police. Data on visits were collected through the NSW Health COVID-19 education and compliance program, which was introduced in June 2020 and coordinated by the NSW Ministry of Health to assist and educate businesses and the community to develop and implement COVID-19 Safety Plans. PHU Environmental Health Officers were tasked with inspecting a set number of businesses within their local health district. The data from the inspections was collected using a universal checklist and entered weekly by each PHU into a secure online Excel database managed centrally by the NSW Ministry of Health, to which all PHUs had access.
Campaign results
Raising community awareness
Diversity Hub cultural support workers engaged face-to-face with the community by undertaking concierge functions at the pop-up clinic, visiting shops, undertaking cultural engagement and delivering in-language posters for display on shopfronts. Anecdotally, the local business owners and shop staff appreciated receiving in-language resources and in-person support from cultural support workers. In addition to social media posts displayed on the SLHD Facebook page, a short English-language Facebook video was produced by SLHD staff to encourage testing for people who had been to Lakemba and developed any flu-like symptoms. The video was viewed on Facebook more than 2100 times between 18 October 2020 and March 2021.
Meetings with religious leaders were organised by senior PHU doctors and other members of the PHU team and held at community places of worship where possible, involving representatives from the Lebanese Muslim Association, Lakemba Mosque, All Saints Greek Orthodox Church, Masjid As-Sunnah Mosque, St Therese Catholic Church and Uniting Church Lakemba (including the Fijian and Korean congregations). Meetings were informal and served to inform the leaders of the current situation regarding the outbreak and how they could support their community. Religious leaders were encouraged to act as ‘COVID Safe champions’ or information intermediaries by delivering COVID-safe messages to their congregations, holding Zoom video platform gatherings where feasible and requesting the community to present for testing. Based on anecdotal feedback from those involved, religious leaders were very responsive and showed an interest in assisting.
Pop-up clinic and testing information
The pop-up testing clinic was run at Lakemba Uniting Church from 13–24 October 2020 and was staffed with SLHD cultural support workers to support attendees. There were 737 COVID-19 tests conducted at the clinic during the campaign. There were 5129 tests performed at nearby pre-existing test locations (Canterbury Hospital Emergency Department, Canterbury COVID-19 Drive-Through Clinic, Roselands Drive-Through Clinic, Lakemba Respiratory Clinic and Belmore Respiratory Clinic) from 12–25 October 2020. Figure 1 shows COVID-19 testing numbers for the local population for the week preceding the campaign (4–11 October) and during the campaign period (12–25 October). The average number of tests per day in the 8 days prior to the commencement of the campaign was 224, and the average number of tests per day during the two-week campaign period was 419, demonstrating an 87% increase in testing numbers in the Lakemba area during the outbreak/campaign.
Figure 1. Daily number of COVID-19 tests taken in Canterbury area, 4–25 October, 2020 (Click figure to enlarge)
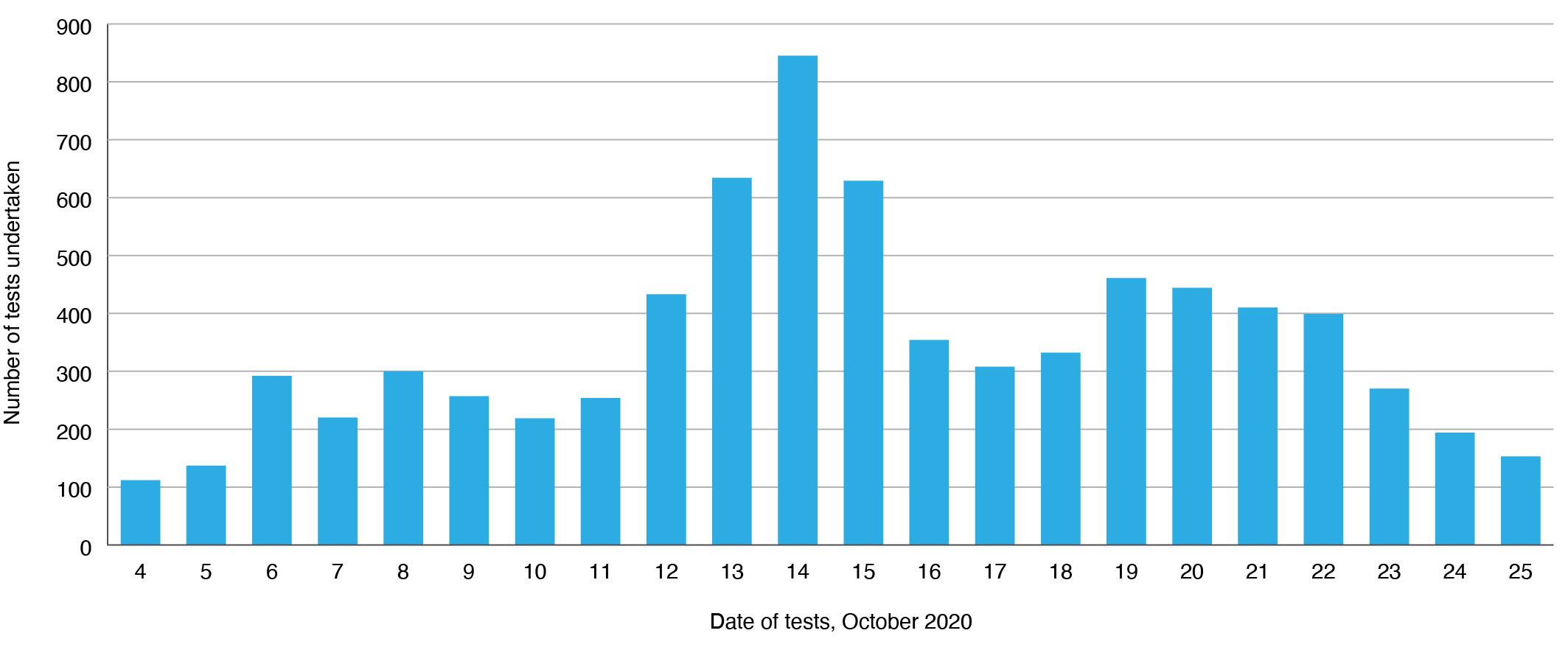
Source: Public Health Response Branch, NSW Health
Supporting local businesses
Agencies undertook 127 visits to local businesses from 15–25 October 2020. NSW Fair Trading conducted gym, beauty and massage parlour visits; café and restaurant visits were conducted by NSW Food Authority/Department of Primary Industries; licensed venue visits were conducted by Liquor and Gaming NSW, and pharmacy and retail visits were conducted by SafeWork NSW. Penalty Infringement Notices were recommended in five of the 127 inspections (4%). There were no referrals made to NSW Health or NSW Police. Due to the nature of the campaign, which formed part of a larger NSW Health COVID education and compliance program, no follow-up data was available to determine whether COVID-safe compliance improved as a result of the campaign.
Lessons learnt
CALD communities are at risk of missing out on key health messages during the COVID-19 pandemic.7,8 Barriers to accessing COVID-19 information include slow translation of health information, gaps in the languages covered by translations and mismatch between information provided and levels of community health literacy.11 Gaps may be filled by information from people’s country of origin, which may not align with local health advice.11 Promisingly, however, community and religious leaders in CALD communities can act as ‘gatekeepers’ or information intermediaries to promote the communication of public health information.12 The Lakemba campaign is an important real-world example of how effective engagement with CALD communities can be undertaken rapidly in a pandemic setting. The campaign encompassed a wide range of community-focused public health measures, including: the provision of a local pop-up testing clinic with cultural liaison staff to mitigate potential barriers to testing; visits to a wide range of local businesses as an opportunity for education; various forms of in-language information; and engagement with local community leaders as ‘COVID Safe’ champions.
While it is impossible to draw causal associations between the campaign activities and the outcome of the Lakemba outbreak, the localised increase in testing numbers during that campaign is a marker of the success of the overall public health response. Further, despite 890 close contacts being identified during the outbreak, only 17 confirmed cases of COVID-19 were detected, demonstrating effective public health management of what could have been a widespread community outbreak. Factors outside the campaign that contributed to the success of the outbreak response included timely contact tracing by the NSW Health Close Contact Tracing Team and SLHD PHU, with ongoing follow-up of identified close contacts during their quarantine period to ensure compliance with quarantine requirements. The Central and Eastern Sydney Primary Health Network (CESPHN) also supported the local medical centres involved in the outbreak and released a health promotion video by a well-known community doctor on social media in Arabic and English (impact unmeasured). There was widespread coverage of the outbreak in mass media and through the NSW Health website.
One key limitation of this report is the inability to undertake a more granular analysis of the campaign’s impact, in particular, the outcomes of the inspections of local businesses. This is due to variations in the data collected by different agencies involved in the campaign. A more streamlined approach with predetermined data fields would enhance impact measurement in future similar campaigns. After the campaign, an integrated collection and reporting tool was developed and applied across all agencies and inspection programs.
Practical lessons were highlighted in a multi-agency debrief at the conclusion of the campaign. Although the campaign was successfully executed in a rapid timeframe (2 days from outbreak commencement to campaign start), participating agencies felt that having a duty roster of two to three staff available for urgent mobilisation at each agency could have further aided rapid deployment. Those involved also felt it would have been beneficial for participating agencies to pre-identify staff with relevant language skills and to prepare templates for community information to allow for expedited resource development. Due to the speed of the campaign, there was insufficient time for more extensive local community engagement in developing the resources used. However, the in-language information developed by SLHD for this purpose included rapid group feedback from relevant communities and was deemed to be of sufficiently high quality to be subsequently adopted by NSW Health for broader use.
Across the world, the differential impact of COVID-19 on vulnerable populations is being demonstrated.4 We have learnt that simply providing translated health information to our CALD communities is not enough to mitigate the inequitable outcomes of the virus in these communities.11 In NSW, a major reason behind the successful suppression of local outbreaks during the early stages of the pandemic was a strong contact tracing system and flexible, localised public health responses. The Lakemba campaign is a unique example of the importance of rapid, multi-agency collaboration and community partnership to ensure an equitable public health response in a pandemic setting.
Peer review and provenance
Externally peer reviewed, not commissioned.
Copyright:

© 2022 Ioannides et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. O’Sullivan D, Rahamathulla M, Pawar M. The impact and implications of COVID-19: an Australian perspective. Int J Community Soc Dev. 2020;2(2):134–51. CrossRef
- 2. Bennett C. Where did Victoria go so wrong with contact tracing, and have they fixed it? Melbourne: The Conversation; 13 Oct 2020 [cited 2022 Sept 30]. Available from theconversation.com/where-did-victoria-go-so-wrong-with-contact-tracing-and-have-they-fixed-it-147993
- 3. McAnulty JM, Ward K. Suppressing the epidemic in New South Wales. N Engl J Med. 2020;382(21):e74. CrossRef | PubMed
- 4. Bambra C, Riordan R, Ford J, Matthews F. The COVID-19 pandemic and health inequalities. J Epidemiol Community Health. 2020;74(11):964–8. CrossRef | PubMed
- 5. Wild A, Kunstler B, Goodwin D, Onyala S, Zhang L, Kufi M, et al. Communicating COVID-19 health information to culturally and linguistically diverse communities: insights from a participatory research collaboration. Public Health Res Pract. 2021;31(1):e3112105. CrossRef | PubMed
- 6. NSW Health. COVID-19 Weekly Surveillance in NSW. Epidemiological week 40, ending 3 October 2020. Sydney; NSW Health; 2020 [cited 2022 Sept 30]. Available from: www.health.nsw.gov.au/Infectious/covid-19/Documents/covid-19-surveillance-report-20201009.pdf
- 7. Australian Bureau of Statistics. Lakemba 2016 Census All person QuickStats. Canberra; ABS; 2016 [cited 2022 Sep 30]. Available from: www.abs.gov.au/census/find-census-data/quickstats/2016/SSC12257
- 8. Smith JA, Judd J. COVID-19: vulnerability and the power of privilege in a pandemic. Health Promot J Austr. 2020;31(2):158–60. CrossRef | PubMed
- 9. Kayman H, Ablorh-Odjidja A. Revisiting public health preparedness: incorporating social justice principles into pandemic preparedness planning for influenza. J Public Heal Manag Pract. 2006;12(4):373–80. CrossRef | PubMed
- 10. Nutbeam D. The vital role of meaningful community engagement in responding to the COVID-19 pandemic. Public Health Res Pract. 2021;31(1):e3112101. CrossRef | PubMed
- 11. Seale H, Harris-Roxas B, Heywood A, Abdi I, Mahimbo A, Chauhan A, Woodland L. Speaking COVID-19: supporting COVID-19 communication and engagement efforts with people from culturally and linguistically diverse communities. BMC Public Health. 2022;22(1);1257. CrossRef | PubMed
- 12. Seale H, Harris-Roxas B, Heywood A, Abdi I, Mahimbo A, Chahan A, Woodland L. The role of community leaders and other information intermediaries during the COVID-19 pandemic: insights from the multicultural sector in Australia. Humanit Soc Sci Commun 2022;9:174. CrossRef