Abstract
Objectives: In response to the coronavirus 2019 (COVID-19) pandemic, a research project was developed with a cohort of 45 and Up Study participants to generate timely, relevant evidence to guide policy, practice and planning. This paper describes the research model, the cohort establishment and characteristics, and some findings.
Methods: A subgroup of 45 and Up Study participants was invited to enrol in 45 and Up COVID Insights –a series of five online surveys conducted during 2020–22. The model involved a close collaborative partnership with the New South Wales Ministry of Health and a panel of scientific advisers, an agile data collection methodology and rapid dissemination of findings. Frequent, iterative engagement with stakeholders provided a framework for identifying survey themes and questions and ensured wide dissemination of findings. Themes included healthcare use, attitudes toward and uptake of COVID-19 prevention measures, and the impact of the pandemic on mental health, loneliness, and lifestyle behaviours.
Results: 45 and Up COVID Insights achieved strong stakeholder engagement through extensive consultation and rapid reporting of results. The project recruited a diverse cohort of 32 115 participants: median age 68 years (range: 56–100+); 8% from outer regional/remote areas; 12% from the most socioeconomically disadvantaged communities; and 9% from culturally and linguistically diverse backgrounds. The first four surveys found that the impact of the pandemic varied across populations and stages of the pandemic.
Between February–April (survey 2) 2021, 10% reported missed healthcare in the past month because of the pandemic, rising to 26% by September–November 2021 (survey 4). Quality of life remained high (>90% good–excellent across the surveys). As the pandemic progressed, the proportion reporting worsened mental health as a result increased from 29% (July–December 2020, survey 1) to 46% (survey 4). In survey 2 (February–April 2021), 89% intended to get the COVID-19 vaccine, with 8% unsure. By late 2021, vaccination uptake was high, with 98% of respondents having received at least one vaccination.
Conclusion: There is great value in harnessing a large longitudinal, well-described, and diverse cohort study to generate evidence in a changing context with evolving information needs. The collaborative model enhanced the value and relevance of the data to inform decisions.
Full text
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has presented unprecedented challenges for decision-makers and researchers. Decision makers are grappling with complex decisions based on uncertain, emerging, changing or even conflicting evidence1,2, while researchers have had to pivot agendas and quickly mobilise their expertise to generate relevant and reliable evidence.3,4
Challenges notwithstanding, the pandemic has presented a new opportunity for researchers and policy makers to work together: cultivating partnerships, coordinating responses, developing shared agendas and forging new ways of working together.5 Collaborative approaches, where researchers and policy makers share resources and identify mutual priorities, have thrived. To this end, communication is critical, ensuring evidence and information gaps are identified and new knowledge is generated and translated efficiently.6
During the pandemic, there was an increase in the prominence and recognition of scientific experts and evidence and the important role they play in informing decision making. Equally, the ability of existing health and research infrastructure to respond with timely evidence was critical. Some key examples include: the National Centre for Immunisation Research and Surveillance gave timely evidence to inform decisions around school operations during the pandemic7,8; the Australian Health Protection Principal Committee issued advice on policies, standards and protections for the general public, including social distancing measures, public gathering rules, travel restrictions and testing criteria9; the Doherty Institute and the University of Sydney contributed to modelling efforts that supported planning for severity and duration of lockdowns10; and the Australian Technical Advisory Group on Immunisation advised on vaccine program implementation, issues and clinical guidance.11
In response to the pandemic and supported by a New South Wales (NSW) Health COVID-19 research grant12, researchers from the Sax Institute’s 45 and Up Study developed a rapid research model. The model involved collaboration between researchers and policy makers and aimed to generate timely, relevant evidence to guide decision making during the pandemic. This paper describes the 45 and Up COVID Insights (hereafter described as COVID Insights) model, outlines the establishment and key characteristics of its cohort and presents some descriptive findings from the first four surveys in the series.
Methods
The 45 and Up Study (the Study) is Australia’s largest longitudinal cohort study of health and ageing. The Study recruited 267 357 participants aged 45 and older from NSW, Australia from 2005 to 2009. Prospective participants were randomly sampled from the Australian Government’s Services Australia Medicare enrolment database. People 80 years and older, and residents of rural and remote areas, were oversampled. Participants were enrolled after completing a questionnaire and giving signed consent to join the Study and have their survey data linked to a broad range of other data sources. This represented about 19% of those invited and 11% of the NSW population aged 45 years and older.13,14 Participants consented to being contacted for 5-yearly follow up surveys and other research projects.
Research model
In mid–2020, as the pandemic emerged, we established COVID Insights, recruiting a subcohort of Study participants to provide timely evidence to guide COVID-relevant decision making. The research model involved three components (detailed below):
1. Collaborative design
The collaborative research model was established via an informal leadership group (including the project team and key policy makers from NSW Health) and a scientific advisory group, which drew from the broad membership of the Sax Institute, which includes leading research groups, universities and other organisations in public health and health research. An ongoing iterative dialogue between the collaborating groups and extensive consultations with stakeholders created a successful collaboration. We engaged widely with clinical, governance and operational networks responding to the pandemic15 in both state and national agencies, with more than 200 stakeholders consulted to inform survey design across the series. These consultations helped development of the surveys by identifying research priorities, which were refined and translated into questionnaires by the project team. This process was complemented by approximately quarterly consultations with a scientific advisory group that advised on methods and measures.
2. Agile data collection
With the course of the pandemic unknown, we developed a series of five rapid surveys intended to measure the impact of the pandemic at different time points. Data collection was designed to be responsive to information needs and conducted in accordance with stakeholder priorities.
3. Rapid reporting
On completion of each data collection cycle, descriptive analyses were available to stakeholders within 2–3 weeks. We conducted 26 forums to present high-level findings (from the first four surveys), which were tailored to the interests of each group and designed to stimulate priority setting for subsequent surveys.
Rapid surveys
Recruitment
From November 2020 to April 2021, 88 840 participants from the Study were invited into the COVID Insights program through two processes. Invitations were sent to 1) respondents from the 2020 routine follow-up survey who indicated interest in contributing to COVID-19 research (n = 28 840). The 2020 follow-up included a COVID supplement which provided data for the first COVID Insights survey; 2) a random selection of remaining study participants contactable by email (n = 40 000) or post only (n = 20 000). Participants who had withdrawn from the Study, died before 20 October 2020 or lived outside NSW, were excluded.
Participants enrolled in COVID Insights by completing online consent, nominating a preferred email or mobile number for follow-up, and completing the first survey.
Data collection
Apart from the initial 2020 COVID Supplement survey, all COVID Insights surveys were conducted online using the REDCap online data platform16 and took around 10 minutes to complete. At the time of writing, four rapid surveys had been completed, with the final survey in the field (March 2022). Table 1 outlines survey themes and timing.
Table 1. Survey themes and timing of initial 45 and Up Study COVID Insights rapid surveys
| Survey themes | Survey 1 Jul–Dec 2020a |
Survey 2 Feb–Apr 2021 |
Survey 3 Jun–Aug 2021 |
Survey 4 Sep–Nov 2021 |
| Healthcare utilisation | ||||
| Missed/delayed healthcare | ✓ | ✓ | ✓ | ✓ |
| Telehealth | ✓ | x | x | ✓ |
| Mental health and wellbeing | ||||
| Impact of pandemic on mental health | ✓ | ✓ | ✓ | ✓ |
| Kessler 6 psychological distress17 | ✓ | x | ✓ | x |
| LTE-Q significant life events18 | x | x | ✓ | x |
| De Jong Gierveld loneliness scale19 | ✓ | x | ✓ | x |
| Financial | ||||
| Impacts | ✓ | x | ✓ | x |
| Stress | x | x | ✓ | x |
| COVID-19 prevention | ||||
| Mask wearing | ✓ | ✓ | ✓ | ✓ |
| Social distancing | ✓ | x | x | x |
| Checking-in to venues | x | x | ✓ | x |
| COVID-19 testing | ✓ | ✓ | ✓ | ✓ |
| COVID-19 vaccination | x | ✓ | ✓ | ✓ |
| Lifestyle behaviours | ||||
| Physical activity | ✓ | x | x | x |
| Alcohol consumption | ✓ | x | x | x |
a Includes responses from the 2020 follow-up COVID Supplement (July–December 2020) of enrolled COVID Insights participants:.
✓ = topic included in survey
x = topic not included in survey
Measures
Throughout the series we employed validated measures where possible. The Kessler 6 measured psychological distress17, the De Jong Gierveld Scale was used to measure loneliness18 and a modified version of ‘The list of threatening experiences’ was used to identify experience of life stressors.19 Other questions were adapted from Study core questionnaires and other existing surveys. World Health Organization questions on behavioural and social drivers of vaccination20 were used as a basis for developing COVID-19 vaccination questions, with some modified to align with a Victorian survey of healthcare workers.21 Questions were developed specifically for COVID Insights using external consultation with theme experts and internal user testing. As the pandemic evolved, pragmatic modifications to questions were required to reflect changing contexts and emerging needs. For example, a question about changes “since the beginning of the pandemic” included in survey 1 required revision as the pandemic progressed to: “in the last week/month”. Full details are available in the COVID Data Hub data dictionary.22
Ethics
The 45 and Up Study and 45 and Up COVID Insights are both approved by the UNSW Sydney Human Research Ethics Committee (references HC210602 and HC200597 respectively).
Responding to evolving information needs
Each COVID Insights survey reflected the evidence and information needs identified by policy and research partners at the time of development. Some questions were repeated across surveys to enable tracking over time. At the time of writing, there had been four periods of the pandemic in NSW where data were collected (Figure 1).
Figure 1. COVID-19 pandemic in NSW – timeline of key events, data collection and four pandemic periods 2020–21 (click figure to enlarge)
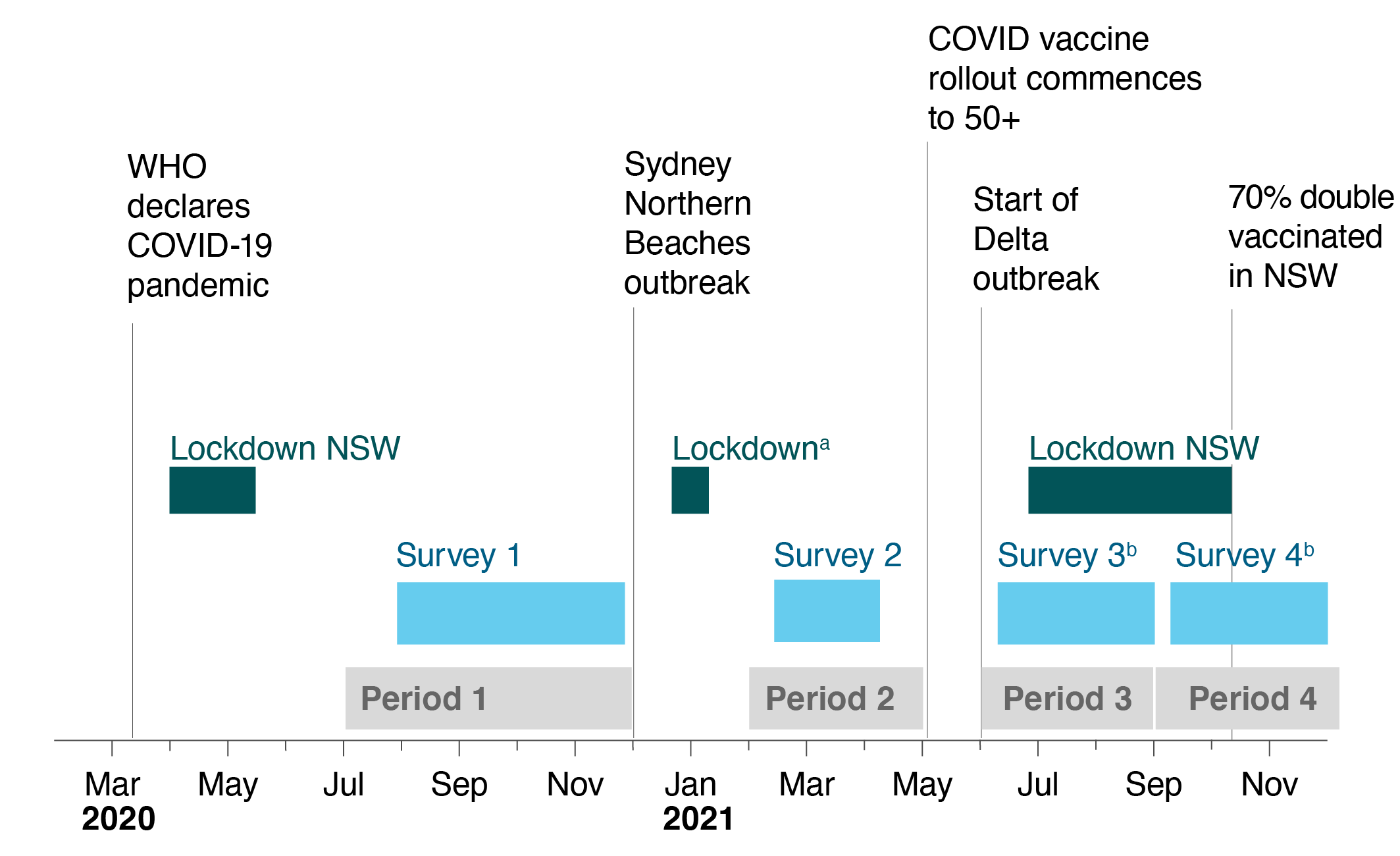
a Lockdown in place across Sydney’s Northern Beaches with some restrictions for Greater Sydney
b Data collected in three consecutive month-long tranches
WHO = World Health Organization
In Australia, restrictions were implemented from mid-March 2020 to curb the first wave of the pandemic and included a stay-at-home order, restrictions on gatherings and bans on certain public premises (outdoor gyms, playgrounds, etc.). In the second half of 2020, when survey 1 began, restrictions were easing in NSW. Stakeholder consultations held throughout September 2020 identified information gaps and priorities including: the impact of the pandemic on lifestyle behaviours; healthcare access; mental health; loneliness; finances; COVID-19 prevention; and attitudes toward a COVID-19 vaccine.
In early 2021, the pandemic response entered a new phase focused on managing small, localised outbreaks and preparing for the COVID-19 vaccine rollout. Stage 1 of the vaccine rollout began in February targeting essential workers (healthcare, quarantine, aged care and border workers), as well as residents in aged care. This was extended to people aged 50 and older in May 2021. Survey 2 explored attitudes and intentions towards the COVID-19 vaccine to identify likely uptake and associated barriers, a key priority for stakeholders at this time.
By mid-2021, the Delta COVID-19 variant was taking hold in NSW. Greater Sydney was under stay-at-home orders from 26 June, with the whole state in lockdown from 18 August 2021. NSW was recording higher case numbers than in previous outbreaks and tougher restrictions were imposed in several areas of Sydney. During this time, there was a need to understand variation in vaccine access and uptake, particularly in areas with high case numbers. There was interest in the impact of restrictions on mental health and the potential compounding effect of cumulative stressors. Stakeholders requested regular updates during this period, so survey 3 was undertaken in three consecutive tranches from June to August.
From September 2021, restrictions were easing as vaccination rates increased. On 11 October, NSW surpassed 70% double-dose vaccination coverage. At this time, stakeholders were interested in maintenance of COVID prevention behaviours post-vaccination as well as a continued focus on healthcare access. Again, data collection for survey 4 was conducted in three consecutive tranches from September to the end of November.
Results
A total of 32 115 participants enrolled in COVID Insights , including 15 252 who completed the 2020 follow-up COVID Supplement and later enrolled in COVID Insights and 16 863 who completed their initial surveys between November and December 2020 (see details in supplementary table 1, available from: figshare.com/articles/dataset/45UpCOVID_Supplementary_Tables_PHRP_2022_pdf/20524827). By survey 4, 554 participants had unsubscribed, withdrawn, died or were not contactable.
Each survey generated insights relevant to the information priorities of that period. Moreover, the cumulative collection of data across the different surveys enabled an understanding of temporal changes in the cohort and subpopulations. Table 2 outlines the baseline descriptive characteristics of the sample.
Table 2. Baseline characteristics of the COVID Insights study population (N = 32 115)
| Characteristic | n (%) |
| Sex | |
| Female | 18 018 (56%) |
| Male | 14 097 (44%) |
| Age | |
| Median (Q1–Q3)a (years) | 68 (63–73) |
| Age range years | 56–100+ |
| 56–64 years | 10 246 (32%) |
| 65–74 years | 15 208 (47%) |
| 75–84 years | 5 931 (18%) |
| 85+ years | 730 (2.3%) |
| Other demographics | |
| Most disadvantaged SEIFA quintileb | 3 851 (12%) |
| Residence in outer regional/remote/very remote areas (ARIA) | 2 624 (8.2%) |
| Culturally and linguistically diversec | 2 793 (8.7%) |
| Aboriginal or Torres Strait Islander | 117 (0.4%) |
| Multimorbidityd | 12 956 (40%) |
| Living in retirement village/aged care | 753 (2.3%) |
a Q1 first quartile, Q3 third quartile.
b Socio-Economic Indexes for Areas (ABS) using Index of Relative Socio-Economic Disadvantage subscale based on most recently reported residential address.
c Not born in a majority English speaking country (Australia, New Zealand, UK, England, Northern Ireland, Scotland, Wales, Ireland, Canada, USA, South Africa) or speaks a language other than English at home.
d Two or more chronic conditions. A chronic condition was identified by the response to the question in any 45 and Up Study survey (2005–2020): “Has a doctor ever told you that you have” cancer (excluding skin cancer, but including the following options: melanoma, breast, prostate or other cancer), cardiovascular disease (heart failure, atrial fibrillation, high blood pressure, other heart disease); stroke, diabetes; asthma; arthritis; Parkinson’s disease; chronic kidney disease. Full details are available summary of all 45 and Up Study Questionnaires.23
Although many themes were included in the COVID Insights surveys, for this paper we present a selection of descriptive results about the impact of the pandemic on missed healthcare, mental health, lifestyle and COVID-19 prevention behaviours. Additional results are available in the supplementary tables, available from figshare.com/articles/dataset/45UpCOVID_Supplementary_Tables_PHRP_2022_pdf/20524827.
Missed healthcare
Between July and December 2020, 41% of respondents reported that ‘as a result of COVID-19 they had missed or delayed healthcare’. Subsequent surveys restricted the time frame to the past month. Across 2021, there was a 16% increase in reporting of missed or delayed healthcare in the past month, from 10% in February–April to 26% in September–November (Supplementary table 2, available from: figshare.com/articles/dataset/45UpCOVID_Supplementary_Tables_PHRP_2022_pdf/20524827). Of note, the phrase “due to the pandemic” was deleted from survey 3 onwards. All surveys showed variation by sex and age, with the highest proportion of missed services reported by women and the youngest age group (56–64 years) (Supplementary table 2, available from: figshare.com/articles/dataset/45UpCOVID_Supplementary_Tables_PHRP_2022_pdf/20524827).
In survey 3, participants were asked about missed cancer screening in the three main population screening programs (breast, bowel and cervical) available for participants up to the age of 75 years. Eight percent of participants in the eligible screening population had missed a cancer screening appointment (breast 9%; cervical 3%; and bowel 3%) because of the pandemic.
Mental health and wellbeing
Across the surveys a high proportion of participants reported their overall quality of life was excellent, very good or good (94–96%) (Figure 2). As the pandemic continued, more people responded that their mental health had worsened as a result (29% in survey 1, rising to 46% in survey 4).
The Kessler 6 scale was used as a self-report measure of psychological distress.17 Kessler 6 scores indicated 12% of participants were experiencing moderate to high psychological distress in survey 1 in late 2020, increasing to 16% in survey 3 in June–September 2021.
The De Jong Gierveld scale was used to assess loneliness.18 Almost one in 10 respondents (9%) experienced intense loneliness in survey 1 and this remained fairly static across the series.
Lifestyle
General lifestyle questions were asked in late 2020. Participants were asked to report how their lifestyle compared with 12 months earlier, 25% of participants reported spending less time on overall physical activity and 25% reported spending more time watching television. However, 16% said they had spent more time on physical activity overall.
COVID-19 prevention (mask wearing, testing and vaccination)
COVID-19 prevention behaviours such as mask wearing and COVID-19 testing showed increased uptake across the four surveys. Mask wearing showed a sharp increase in June 2021 when masks became mandatory in NSW during the Delta outbreak, remaining consistently high to the end of survey 4 (Figure 2).
Intention to get a COVID-19 vaccination and uptake of vaccination also trended upwards across the surveys (Figure 2). At the height of the Delta outbreak in NSW, survey 3 showed vaccine uptake increased to 84%, with a further 11% of respondents planning to vaccinate By completion of survey 4 at the end of November 2021, 98% of respondents had received at least one vaccination, and a further 0.5% intended to get vaccinated (Supplementary table 2, available from: figshare.com/articles/dataset/45UpCOVID_Supplementary_Tables_PHRP_2022_pdf/20524827).
Figure 2. Prevalence of COVID-19 health and prevention measures with 95% confidence intervals, by surveya (click figure to enlarge)
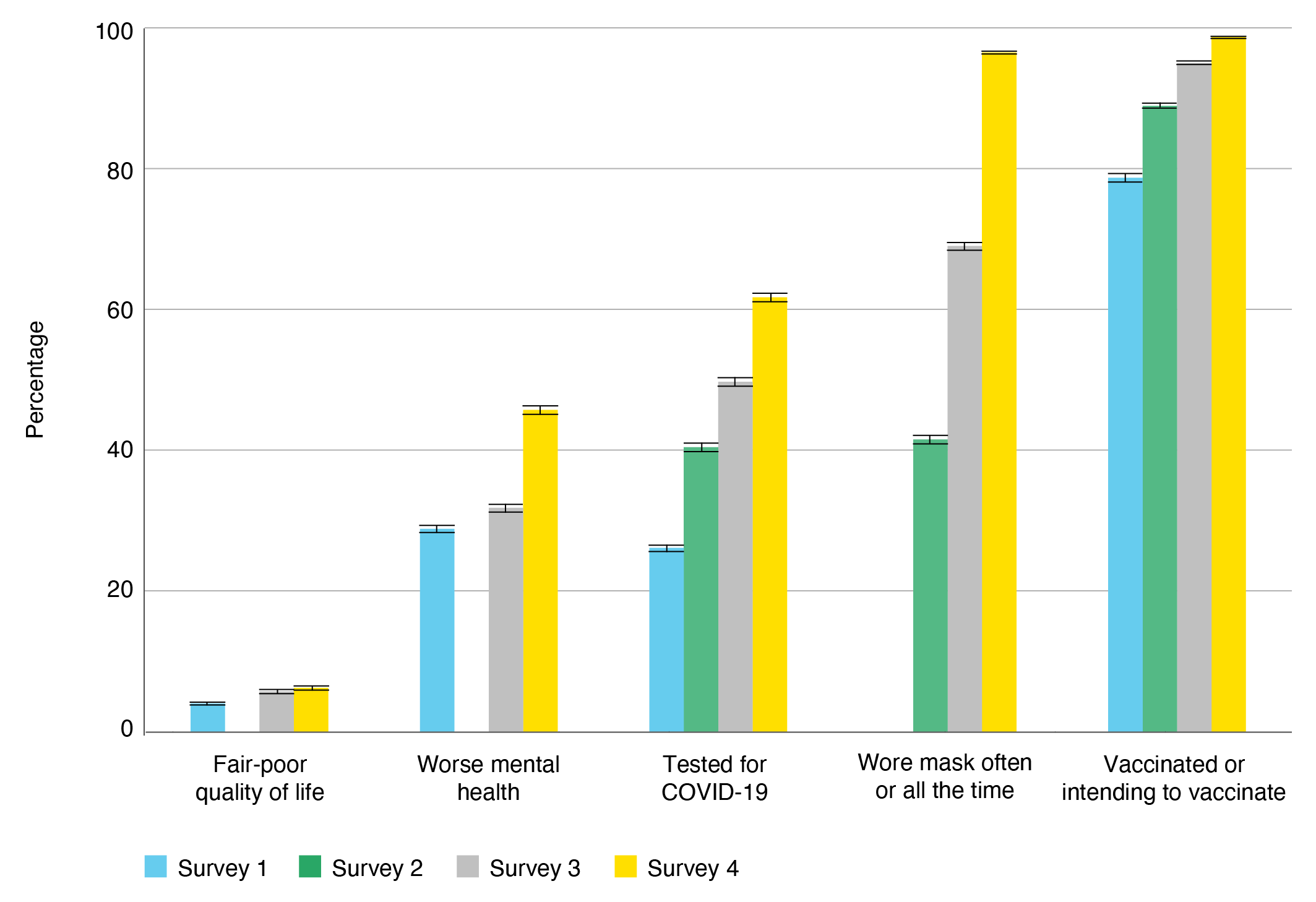
a Questions on quality of life were not included in survey 2. Questions on mental health were phrased differently in survey 2 and were not comparable across the surveys.
Discussion
The COVID Insights project demonstrates the capacity of a large, longitudinal study to develop responsive approaches to generating evidence. The collaborative model provided a framework for continued engagement and consultation with stakeholders, ensuring data collection was relevant and aligned to information needs. The agile methodology and rapid reporting mechanisms reduced the lengthy time frames typically associated with study design, governance, data collection, analysis and reporting, enabling timely delivery of results. Our findings illustrate how uptake of COVID-19 prevention measures, including vaccination, changed over time and enabled us to track missed/delayed healthcare. The mental health impacts of the pandemic were notable, with more participants reporting worse mental health as the pandemic progressed with marked disparities in some subgroups.
Policy decisions are usually informed by multiple inputs, making it difficult to discern the impact of our findings. Nonetheless, multiple requests for information and feedback from stakeholders suggested our findings were considered in decision-making processes in response to COVID-19. For example, evidence from our surveys on the experience of loneliness for people living alone was called on by mental health researchers to advocate for the introduction of ‘singles bubbles’ during lockdown.24 Cancer agencies also reported that findings relating to missed cancer screening were important for planning and were an important flag for delayed diagnoses. Information on missed healthcare was recognised as particularly valuable because it was not available from other sources. The data also identified population subgroups particularly affected by the pandemic, informing targeted responses.
Limitations
Although the study sample was diverse, large and had a high response rate, several limitations need to be acknowledged. These include: 1) no representation of younger populations (the youngest participant in our study was aged 56); 2) surveys were conducted online, resulting in a more technologically savvy cohort; 3) surveys were only conducted in English, limiting participation to people with sufficient English proficiency; 4) most participants (99%) were living in NSW and, because COVID-19 outbreaks and government responses varied markedly across Australia and internationally during the pandemic, the impact on residents would also have varied; 5) the phrasing in some questions was changed in response to changes in context and feedback from stakeholders, which may affect comparability across time; and 6) the rapid development and implementation of surveys also minimised opportunities for extensive user testing. Moreover, it should be emphasised that the Study was not designed to be representative of the general older population in NSW and therefore does not provide population-level measures of incidence and prevalence.13,14,25
Strengths
Key strengths include: 1) the capacity of the research to be responsive to a changing context and deliver timely and relevant evidence for planning and decision making; 2) the large and diverse nature of the older cohort who live across metropolitan and regional areas of NSW; 3) the ability to link to data collected since the Study began (2005–2009); 4) the diverse health and care needs; 5) varied lifestyles; and 6) inclusion of very old people with no upper age limit. The large sample size supports categorisation into subcohorts to understand variation in different populations. A subgroup/stratum size of at least 3000 allows stratum-specific estimates of proportions with 95% confidence intervals within ± 2% for proportions and ± 0.05 standard deviations for means and differences in characteristics between exposed and unexposed groups of 2%–10% for proportions and 0.1–0.25 standard deviations for means, with ratios of sample size between groups of 1:1 to 20:1.
Data from COVID Insights will be incorporated into the 15 years of Study data on lifestyles, social circumstances, health and wellbeing, and healthcare use, which can be linked to other routinely collected data, identifying outcomes, healthcare use, new conditions, vaccine uptake, mortality and much more. The Study is a resource for all researchers for ethics-approved projects.
The COVID Insights research model is being adopted as the primary methodology in a new research program that will generate evidence to guide decision making over the next few years. The valuable partnerships and collaborations established as part of this project will continue to provide critical channels for communication of key issues and challenges, which we hope can forge better engagement and alignment between research and policy worlds in the future.
Conclusion
Adopting a collaborative research model, along with a rapid survey methodology, enabled us to leverage the Study to respond to the evolving challenges presented by the COVID-19 pandemic. The approach fostered new and existing partnerships with both the academic and policy sectors and promoted a responsive approach to evidence generation and translation. Rapid feedback loops ensured timely delivery of findings, creating avenues for ongoing input into data collection. Anecdotal evidence suggests the findings have been used to inform planning and decision making, and the data on missed healthcare have been recognised as filling an important information gap.
Acknowledgements
The COVID Insights project received funding from the NSW Health COVID Research Grants Round 1. The project has benefited from advice and guidance from the following additional collaborators: Dianne O’Connell, Kirsten McCaffery, Julie Leask, Raina MacIntyre and Julie Redfern.
Authors GD, KB, SB and MM work on the 45 and Up Study as part of their employment with the Sax Institute.
This paper is part of a special issue of PHRP reflecting on the 45 and Up Study. The edition is published in memory of world-renowned epidemiologist Dame Valerie Beral (1946-2022), who played a vital role in establishing and supporting the Study.
The 45 and Up Study is managed by the Sax Institute in collaboration with partners Cancer Council NSW, the Heart Foundation and NSW Ministry of Health.
Peer review and provenance
Externally peer reviewed, not commissioned.
Copyright:

© 2022 Dawson et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Marten R, El-Jardali F, Hafeez A, Hanefeld J, Leung GM, Ghaffar A. Co-producing the covid-19 response in Germany, Hong Kong, Lebanon, and Pakistan. BMJ. 2021;372:n243. CrossRef | PubMed
- 2. Berger L, Berger N, Bosetti V, Gilboa I, Hansen LP, Jarvis C, et al. Rational policymaking during a pandemic. Proc Nat Acad Sci U S A. 2021;118(4):e2012704118. CrossRef | PubMed
- 3. Shapira P. Scientific publications and COVID-19 “research pivots” during the pandemic: an initial bibliometric analysis. bioRxiv. 2020:2020.12.06.413682. CrossRef
- 4. Weiner DL, Balasubramaniam V, Shah SI, Javier JR, on behalf of the Pediatric Policy Council. COVID-19 impact on research, lessons learned from COVID-19 research, implications for pediatric research. Pediatr Res. 2020;88(2):148–50. CrossRef | PubMed
- 5. Rose S, Estes J. Creating effective research-policy partnerships for COVID response and beyond. Washington, DC: Centre for Global Development; 2021 [cited 2021 Dec 3]. Available from: Available from: www.cgdev.org/blog/creating-effective-research-policy-parterships-covid-response-and-beyond
- 6. McMahon M, Nadigel J, Thompson E, Glazier RH. Informing Canada's health system response to COVID-19: priorities for health services and policy research. Health Policy. 2020;16(1):112–24. CrossRef | PubMed
- 7. Macartney K, Quinn HE, Pillsbury AJ, Koirala A, Deng L, Winkler N, et al. Transmission of SARS-CoV-2 in Australian educational settings: a prospective cohort study. Lancet Child Adolesc Health. 2020;4(11):807–16. CrossRef | PubMed
- 8. Campbell D, Edwards B, Milat A, Thackway S, Whittaker E, Goudswaard L, et al. NSW Health COVID-19 Emergency Response Priority Research program: a case study of rapid translation of research into health decision making. Public Health Res Pract. 2021;31(4): 3142124. CrossRef | PubMed
- 9. Australian Government Department of Health. Australian Health Protection Principal Committee (AHPPC). Canberra: Australian Government; 2021 [cited 2022 Mar 8]. Available from: Available from: : www.health.gov.au/committees-and-groups/australian-health-protection-principal-committee-ahppc
- 10. Australian Government Department of Prime Minister and Cabinet. Doherty Institute COVID-19 modelling: Key findings and implications – including sensitivity analysis. Canberra: Australian Government; 2021 [cited 2022 Mar 8]. Available from: Available from: www.pmc.gov.au/sites/default/files/files/findings-and-implications-of-doherty-institute-covid-19-modelling-and-sensitivity-analysis-presentation.pdf
- 11. Australian Government Department of Health and Aged Care. Australian Technical Advisory Group on Immunisation (ATAGI). Canberra: Australian Government; 2021 [cited 2022 Mar 8]. Available from: www.health.gov.au/committees-and-groups/australian-technical-advisory-group-on-immunisation-atagi
- 12. NSW Health. 45 and Up COVID Insights: Sax Institute. Sydney: NSW Health; 2020 [cited 2022 Mar 8]. Available from: www.medicalresearch.nsw.gov.au/projects/45-and-up-covid-insights/
- 13. 45 and Up Study Collaborators, Banks E, Redman S, Jorm L, Armstrong B, Bauman A, et al. Cohort profile: the 45 and Up Study. Int J Epidemiol. 2008;37(5):941–7. CrossRef | PubMed
- 14. Bleicher K, Summerhayes R, Baynes S, Swarbrick M, Navin Cristina T, Luc H, et al. Cohort Profile Update: the 45 and Up Study. Int J Epidemiol. 2022;dyac104. Online ahead of print. CrossRef | PubMed
- 15. Levesque J-F, Sutherland K, Watson DE, Currow DC, Bolevich Z, Koff E. Learning systems in times of crisis: the Covid-19 critical intelligence unit in New South Wales, Australia. NEJM Catalyst. 2020;1(6). • Article
- 16. REDCap. Project REDcap. Nashville, TN: REDCap; [cited 2022 March 8]. Available from: Available from: www.project-redcap.org
- 17. Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normand SL, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–76. CrossRef | PubMed
- 18. De Jong Gierveld J, Van Tilburg T. The De Jong Gierveld short scales for emotional and social loneliness: tested on data from 7 countries in the UN generations and gender surveys. Eur J Ageing. 2010;7(2):121–30. CrossRef | PubMed
- 19 Brugha TS, Cragg D. The list of threatening experiences: the reliability and validity of a brief life events questionnaire. Acta Psychiatr Scand. 1990;82(1):77–81. CrossRef | PubMed
- 20. World Health Organization. Data for action: achieving high uptake of COVID-19 vaccines: interim guidance April 2021. Geneva: WHO; 2021 [cited 2022 Mar 25]. Available from: www.who.int/publications/i/item/WHO-2019-nCoV-vaccination-demand-planning-2021.1
- 21. Murdoch Children’s Research Institute (MCRI), University of Melbourne, University of New South Wales, Monash University, University of Sydney. The COVID vaccine preparedness study – summary of report for the Victorian Government, 14 May 2021. Melbourne: Victoria State Government; 2021 [cited 2022 Mar 25]. Available from: www.mcri.edu.au/images/documents/migrate/covid_vaccine_preparedness_study_-_summary_of_results_25_6_21.pdf
- 22. Sax Institute. COVID Data Hub data dictionary. Sydney: Sax Institute; 2022. [cited 2022 Aug 15]. Available from: www.saxinstitute.org.au/our-work/45-up-study/data-book/
- 23. Sax Institute. Summary of all 45 and Up Study questionnaires. Sydney: Sax Institute. 2021 [cited 2022 Aug 18]. Available from www.saxinstitute.org.au/our-work/45-up-study/questionnaires/
- 24. Black Dog Institute. The Black Dog Institute urges NSW Government to introduce ‘single’s bubble’. Sydney: Black Dog Institute; 2021 [cited 2021 Nov 28]. Available from: www.blackdoginstitute.org.au/media-releases/the-black-dog-institute-urges-nsw-government-to-introduce-singles-bubble/
- 25. Mealing NM, Banks E, Jorm LR, Steel DG, Clements MS. Investigation of relative risk estimates from studies of the same population with contrasting response rates and designs. BMC Med Res Methodol. 2010;10:26. CrossRef | PubMed