Abstract
Background/objective: Co-production is a collaborative method that can make the research process more egalitarian by ensuring researchers work in partnership with key stakeholders in both the design and delivery of research projects and outcomes. A departure from more traditional ways of conducting research, co-production requires the researcher to reflect on their role in the co-production partnership. However, academic research projects are often constrained by parameters set by funding bodies, ethics committees and the researchers themselves. This raises questions about whether some of the key tenets of co-production, including equally shared power, control and responsibility, can be achieved in a meaningful way. This paper presents some of the issues and challenges faced by researchers in achieving shared power when utilising co-production methodology in academic settings.
Type of program or service: The application of co-production within an academic research project is illustrated by a case study involving co-production with family carers, people living with dementia and service providers to develop dementia-specific training for home care workers.
Results: There were unavoidable external constraints on sharing power and decision making within some elements of this project. Project parameters, including the research topic, timelines and funds available, were set by the funding body. Similarly, the study objectives and methods involving participants were required to be predetermined for ethical review. Power was redistributed by shifting the power dynamic in various ways within the internal project environment. Researchers developed strong relationships and built trust with key stakeholders, maintained consistent communication, negotiated conflict, ensured each stakeholder voice was heard and supported people living with dementia to be involved safely and comfortably.
Lessons learnt: Funding body requirements, ethical governance and researcher responsibilities can limit power sharing and decision making when using co-production in academic contexts. Although the researcher or research organisation may hold ultimate responsibility for the overall management and delivery of the project, power can still be ceded and redistributed at many points within the project.
Full text
Introduction
Co-production can facilitate meaningful and equitable partnerships between researchers and end-users who may include service providers, consumers and policy makers.1 In theory, co-production can redistribute responsibility, power and control between researchers and key stakeholders.2 In this way, it is possible to achieve greater impact from research outcomes as the research design is directly informed by community needs and preferences, outcomes meet community expectations, uptake is more likely, and interventions or programs are more sustainable.3
However, when co-production is undertaken in academic contexts, there are several specific challenges to achieving an equitable collaboration, and more so when the research involves vulnerable communities, such as people living with dementia.4,5 These challenges include building trust and respect in relationships with patients and professionals3, researchers having to ‘give up’ control and power over the research process to a certain extent6, and acknowledging ‘lay’ expertise as a legitimate and valuable contribution to knowledge.7,8
Importantly, the role of the researcher is reconceptualised in the co-production process.9 Researchers must adjust to a new researcher–participant relationship, one where rather than being passively ‘studied; by the researcher, participants actively contribute to the research outcomes.10 At the same time, responsibilities such as designing scientifically sound projects, attracting research funding, adhering to the ethical conduct of research, protecting participants from harm, and ultimately, holding overall responsibility for the delivery of a project remain with researchers. Thus there may be several sticking points between traditional research paradigms and new forms of co-production. Co-production challenges the top-down knowledge production hierarchy of traditional academic research.11 This raises questions about how the aims of co-production fit within existing power differentials and how sharing power across the research decision-making process is influenced by the current academic environment.
This paper aims to answer these questions by examining factors within the wider funding, ethics and governance context that may influence the power differentials in the co-production collaboration. Using our project, Promoting Independence Through quality dementia Care in the Home (PITCH), as a case study, we focus on the issues related to using co-production in academic research and challenges for researchers when producing and delivering a research project that seeks to improve the lives of people living with dementia through developing dementia-specific training for home care workers.
The PITCH project
The PITCH project involved co-producing and delivering a training program for home care workers who provide care for people living with dementia, followed by a randomised controlled trial (RCT) to assess the effectiveness of the training program. The co-production elements of this project involved four stages (see Figure 1), with the Project Advisory Group acting as co-production partners at different stages of the process. The partners were selected to represent the end-users or ultimate beneficiaries of the research and included:
- People living with dementia and their family carers
- Home care workers
- Home care managers
- Dementia education providers
- Policy makers
- Advocacy groups
- The research team
Figure 1. Co-production in PITCH: Project Advisory Group members involved in each stage of the co-production processa (click on image to enlarge)
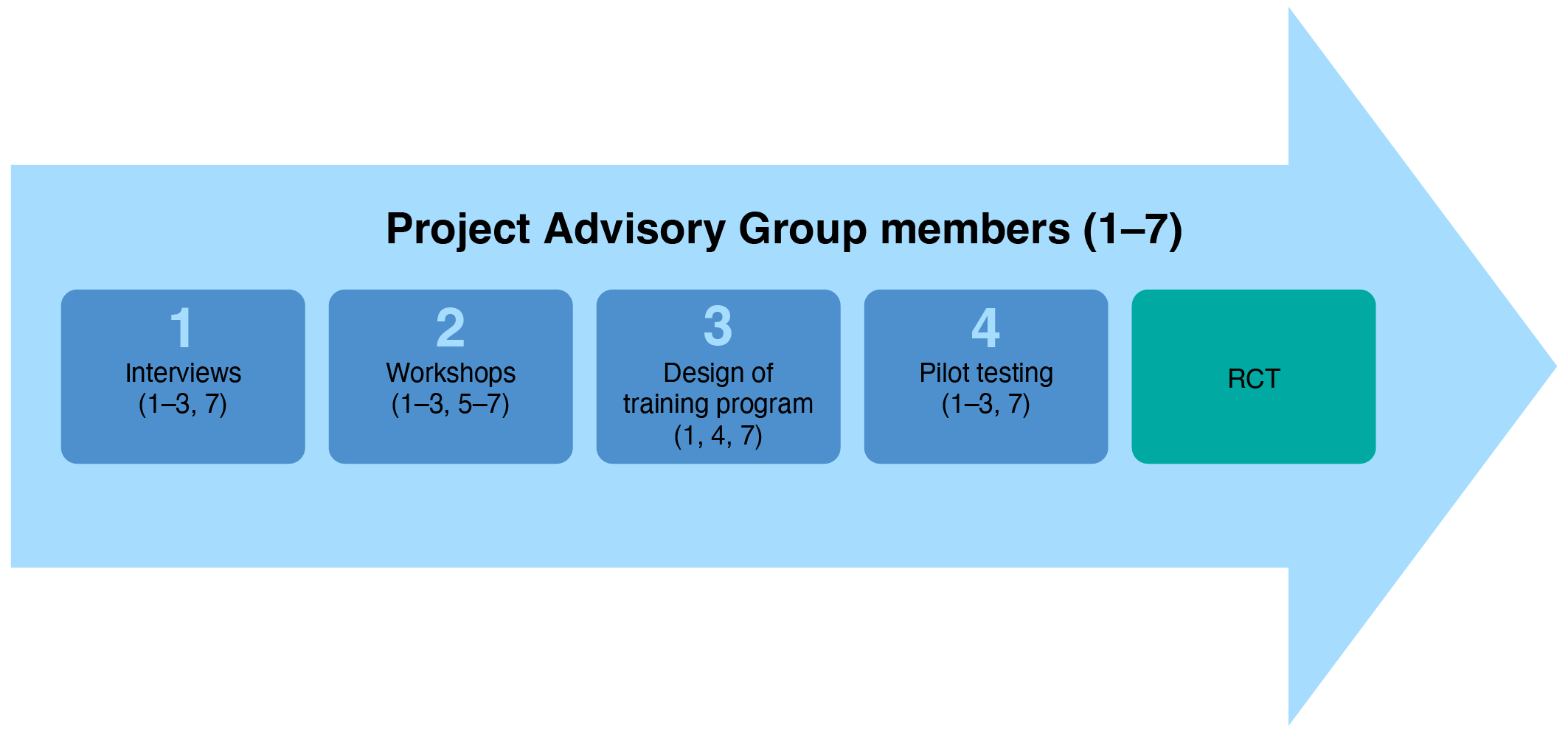
a Project advisory group numbers 1–7 relate to listing in text above.
RCT = Randomised controlled trial
The training program aimed to improve home care workers understanding of their role, their knowledge of dementia as it affects the person’s health and behaviour, the implications of this for their care practices, and how to work effectively as part of a care team with the person with dementia and their family carer/s. The logic behind the PITCH project was that participating in this course would improve knowledge and self-efficacy, ultimately improving care for the person living with dementia. Therefore, it was critically important to include people living with dementia and their carers in the co-design process used to create the content of the training. The co-design framework and process used to develop the PITCH education program, including the involvement of people living with dementia, have been described in detail elsewhere.12 In summary, interviews were conducted to better understand what was important to service users and service providers in quality home care. World café workshops13 were held to generate ideas for the training program, and pilot testing of the prototype training program was conducted with two groups of home care workers and the Project Advisory Group, enabling input from all end-user groups. The PITCH project received ethics approval from the Austin Hospital (HREC17Austin537) and was supported by an Australian National Health and Medical Research Council (NHMRC) grant.
Funding constraints and achieving shared power
Funding for the PITCH project was received through a competitive government grant. Ideally, co-production methods should be used to collectively determine the research priorities and the research agenda. But such an approach can conflict with funding body requirements for study designs to be clearly outlined at the time of funding application. Additionally, outcomes often need to be anticipated at the time of the funding application to present a case for the significance of the research. In short, while funders need specificity – i.e. to know what they are funding – and researchers need to be accountable for the public monies they have been granted, where does that leave consumer input into the research design process?
Co-production can increase the accountability and transparency of the research process and outcomes through public involvement. The public has a right to be involved in and influence how public funds are spent14, including determining research priorities and setting the research agenda. During the development of the grant application for PITCH, a carer advisor who had extensive experience supporting someone living with dementia was consulted on the design of the study. This engagement resulted from an established relationship between the carer advisor and the research organisation. However, it may not always be possible to engage and source payment for consumer advisors at the research design stage, particularly if the project is reliant on securing project-specific funding to provide consumer remuneration. Junior researchers who may not have developed relationships with consumers or have the funds to fairly remunerate consumers for their time may be particularly disadvantaged. Moreover, given the overall low success rates in research funding, the long lead times between funding submissions and notification of outcomes, and the prerequisite legal agreements and project establishment needed before data collection can commence, careful thought must be given to enlisting consumers to extensively input into funding applications as this risks burdening already overstretched end-users.
Risk minimisation versus agency in co-production
The PITCH research was conducted in accordance with the National Health and Medical Research Council (NHMRC) National Statement on Ethical Conduct in Human Research15 and was reviewed and received approval from a human research ethics committee (see above). Ethical review processes are generally designed for top-down research, as emphasis during review is placed on the research questions, study procedures and methods of involvement to determine risk. With co-design and co-production being emergent processes, exact procedures and methods of engaging consumers and other stakeholders are often not known at the time of submitting an application for ethical approval, raising questions about the preparedness of ethics committees to respond to the increase in the use of co-production methods.16 The Project Advisory Group guided the development of the co-design process used to develop the training program. However, the general topics and questions to be presented in the co-design workshops and proposed workshop agendas were required to be reviewed and approved by the ethics committee prior to engaging the wider group of co-designers. While questions were general and allowed for some flexibility when determining the final co-design tools and activities used to generate responses, overall power in shaping the co-production and co-design processes was held by the researcher, under the direction and oversight of the ethics committee.
Sharing power within existing parameters
As the project parameters (e.g. research topic, timelines, and funds available) were set by the funding body, the project objectives largely set by the researchers, and the co-design process required to be predetermined by the ethics committee, how was power ‘shared’ within this collaboration, and was this true sharing? The researchers’ focus was on building strong relationships with the co-designers and developing trust with them. Having a carer chair the Project Advisory Group – a position that would traditionally be held by an academic researcher – was an attempt to share power, develop trust and draw on the carer’s extensive lived experience and expertise. Methods of engagement were designed to privilege the voices of the people living with dementia involved in the project12 and participants were regularly updated about the pilot program and RCT following their involvement in co-designing the training content.
A key strength of the PITCH study was involving people with dementia in co-production and co-design. Although the researchers ultimately had to balance participant agency and autonomy with risk minimisation and protection of a person with dementia as a participant in the research, the PITCH co-production process was designed to facilitate the inclusion of people with a diagnosis of dementia. In the end, two people with a diagnosis of dementia were members of the Project Advisory Group, and four were in the co-design workshops. These numbers may seem low but are encouraging in the context of dementia research, where the direct involvement of people with dementia in social care studies is <10%.17 To facilitate recruitment and sustain retention, members of the research team had clinical qualifications and experience working with people with dementia. Given the potential vulnerability of the group of people involved, all aspects of the co-design process were developed by the research team to enable maximum participation and minimum risk to those living with dementia. Thus, while not able to overcome the power differentials associated with declining cognition and dementia, the research team made every effort to include people with dementia in the study co-production process.
Finally, managing within-group power dynamics through conflict resolution and negotiation was essential in developing trust, as power-sharing is often not only an issue between researchers and end-users but also between end-user groups. For example, there were differences in the extent to which each of the end-user groups could determine the final product (the training program). Despite family carers expressing a preference for a longer program, it needed to be delivered within the existing service system. As such, home care providers had the ultimate say on how long and how often they would release their staff for training. Being transparent about what is and isn’t achievable at the beginning of the co-production process not only works to establish trust but is also important in managing the expectations of the end-user groups.
Conclusion
Using PITCH as a case study, we have highlighted some of the challenges faced by researchers when using co-production in real-world research. A key challenge is whether it is possible to truly share power between researchers and consumers, particularly considering the influence of funding and ethical governance requirements on power differentials in the co-production relationship. We offer no easy answers, instead noting that achieving an equitable co-production relationship and avoiding co-production being undertaken in a token or ‘tick-box’ way requires a redistribution of power within the research partnership. As discussed, this may not always be possible in academia due to the focus commonly being on pre-defined issues and existing power hierarchies within communities rather than the research partnership itself.
Building trust with key stakeholders by developing and maintaining strong and respectful relationships, particularly with vulnerable or hard-to-reach communities, can work towards attenuating some power disparities. It may be that building trust and creating an environment within the co-production relationship where lived experience is valued, and each person’s contribution is respected, can lead to a shift in power dynamics within the traditional researcher-participant relationship. While one step forward is to address the power differential created by consumers’ lack of decision-making capacity, maybe it’s also time to start asking more complex questions about power in the research co-production processes such as: where else is a re-distribution of power required? Engaging vulnerable communities and considering the political, social and ethical considerations of representation and inclusion are foundational to co-design. However, these principles apply not only to research methodologies but also require consideration at other stages in the research pipeline.
Acknowledgements
The PITCH project discussed in the case study was funded by an Australian NHMRC grant.
Peer review and provenance
Externally peer reviewed, invited.
Copyright:

© 2022 Gaffy et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Hickey G, Richards T, Sheehy J. Co-production from proposal to paper. Nature. 2018;562(7725):29–31. CrossRef | PubMed
- 2. Ostrom E. Crossing the great divide: co-production, synergy, and development. World Development. 1996;24(6):1073–87. CrossRef
- 3. Batalden P. Getting more health from healthcare: quality improvement must acknowledge patient coproduction – an essay by Paul Batalden. BMJ. 2018;k3617. CrossRef
- 4. Wang G, Marradi C, Albayrak A, van der Cammen TJ. Co-designing with people with dementia: A scoping review of involving people with dementia in design research. Maturitas. 2019;127:55–63. CrossRef | PubMed
- 5. Hendriks N, Slegers K, Duysburgh P. Codesign with people living with cognitive or sensory impairments: a case for method stories and uniqueness. CoDesign. 2015;11(1):70–82. CrossRef
- 6. Oliver K, Kothari A, Mays N. The dark side of coproduction: do the costs outweigh the benefits for health research? Health Res Policy Syst. 2019;17(1):33. CrossRef | PubMed
- 7. Pols J. Knowing patients: turning patient knowledge into science. Science, Technology, & Human Values. 2014;39(1):73–97. CrossRef
- 8. Williams O, Sarre S, Papoulias SC, Knowles S, Robert G, Beresford P, et al. Lost in the shadows: reflections on the dark side of co-production. Health Res Policy Syst. 2020;18:43. CrossRef | PubMed
- 9. Durose C, Beebeejaun Y, Rees J, Richardson J, Richardson L. Towards co-production in research with communities. Manchester UK: Connected Communities. Arts and Humanities Research Council;2012 [cited 2022 May 30]. Available from: www.research.manchester.ac.uk/portal/files/33424282/FULL_TEXT.PDF
- 10. Sanders EB-N. From user-centered to participatory design approaches. Design and the social sciences: Florida, US: CRC Press; 2002. p. 18–25. CrossRef
- 11. Bell DM, Pahl K. Co-production: towards a utopian approach. Int J Social Res Methodol. 2018;21(1):105–17. CrossRef
- 12. Goh AM, Doyle C, Gaffy E, Batchelor F, Polacsek M, Savvas S, et al. Co-designing a dementia-specific education and training program for home care workers: The 'Promoting Independence Through Quality Dementia Care at Home' project. Dementia (London). 2022;21(3):899–917. CrossRef | PubMed
- 13. The World Café. Design Principles. CA, US: TWC;2021 [cited 2022 May 30]. Available from: www.theworldcafe.com/key-concepts-resources/design-principles/
- 14. Oliver S, Liabo K, Stewart R, Rees R. Public involvement in research: making sense of the diversity. J Health Serv Res Policy. 2015;20(1):45–51. CrossRef | PubMed
- 15. National Health and Medical Research Council. National statement on ethical conduct in human research. Canberra: Australian Government NHMRC; 2007 (updated 2018) [cited 2022 May 30]. Available from: www.nhmrc.gov.au/about-us/publications/national-statement-ethical-conduct-human-research-2007-updated-2018
- 16. Goodyear-Smith F, Jackson C, Greenhalgh T. Co-design and implementation research: challenges and solutions for ethics committees. BMC Med Ethics. 2015;16(1):78. CrossRef | PubMed
- 17. Bartlett R, Milne R, Croucher R. Strategies to improve recruitment of people with dementia to research studies. Dementia (London). 2019;18(7-8):2494–504. CrossRef | PubMed