Abstract
Objective and importance of study: Considerable evidence suggests that adverse social determinants of health (SDH), such as poor education, unemployment, food and housing insecurity, interpersonal violence, inadequate social support and poverty, are key determinants of health and wellbeing. This prospective cohort study piloted a screening tool to collect individual SDH data in a South Australian hospital inpatient population. We explored participants’ attitudes to SDH screening in brief follow-up interviews.
Methods: This mixed-methods study used an SDH screening tool to collect individual-level SDH data from inpatients living in a highly disadvantaged socio-economic area. Participants had a primary diagnosis of chronic obstructive pulmonary disease (COPD), heart failure (HF) or diabetes mellitus. Follow-up interviews were completed post discharge via telephone. Descriptive statistics were employed to examine the prevalence and type of adverse SDH reported by the sample. Thematic analysis was applied to explore participants’ attitudes to the screening.
Results: The sample population (N = 37) reported a substantial burden of a range of adverse SDH (mean 4.7 adverse SDH experienced per participant, standard deviation 2.8). Participants involved in follow-up interviews (n = 8) believed screening might enhance communication between healthcare providers and patients and assist in identifying underlying social problems.
Conclusion: A screening tool for SDH was successfully used to collect individual-level data in a hospital setting. An array of adverse SDH was common in the sample population. Participants believed screening for SDH may potentially benefit doctors and patients. A larger study is required to more robustly characterise the adverse SDH affecting individuals in this population and to explore how the healthcare system might effectively intervene.
Full text
Introduction
Conventional determinants of health, such as pathophysiology and genetics, remain the focus of many national healthcare policies, despite considerable evidence supporting social determinants of health (SDH) as key determinants of health and healthcare outcomes.1 It is well established that health and wellbeing follow a ‘social gradient’: the higher one’s socio-economic status (SES), the longer and healthier they are likely to live.1 Considerable evidence suggests that intervening in adverse SDH, such as food and housing insecurity, or exposure to interpersonal violence and poverty, should be a primary focus of healthcare policy and practice.1,2 SDH interventions in clinical contexts should be tailored to each target population and environment. Generally, they comprise two components: 1) SDH screening, wherein adverse SDH are identified by multidisciplinary healthcare teams and 2) referral to external community organisations to assist with social needs as appropriate. These multidisciplinary teams typically consist of nurses, practitioners and community healthcare workers embedded in healthcare centres. In the context of chronic care, these teams have been associated with decreased hospital inpatient admissions3,4, decreased emergency department admissions3,4, reduced healthcare costs per person3,4 and significant improvements in blood pressure5, lipid levels5 and depression.6
In Australia, systematic action to address adverse SDH in clinical contexts is limited. To date, attitudes of healthcare providers towards SDH interventions have been extensively studied7,8, while those of healthcare users remain largely unexplored.
To fill these gaps, we aimed to 1) develop and pilot a screening tool to systematically collect individual-level SDH data in an inpatient setting, 2) examine the prevalence and types of adverse SDH present in the sample population, and 3) explore participants’ attitudes to screening for SDH.
Methods
A review of SDH literature published 2000–2018 was conducted to identify SDH screening tools currently employed. The screening tool employed in this study was a modified version of the Flinders University Social Health History Screening Tool (FUST)9, used with permission from the authors. The FUST collects data on sociodemographic status, employment, housing stability, internet use, social support, difficulties seeking medical care and exposure to abuse and stress. This tool was initially piloted among 50 participants in a proof-of-concept study; it has not been validated. Further piloting has been recommended across various clinical settings to determine its efficacy.9 For the purpose of our study, we made minor modifications to the tool, simplifying the language of some questions to help participants understand the nature of the questions.
The study took place from July 2017 to May 2019 and ethics approval was obtained from the Central Adelaide Local Health Network Human Research Ethics Committee (HREC/17/TQEH/81). Screening for adverse SDH took place at the Lyell McEwin Hospital (LMH), a major tertiary hospital in the Northern Adelaide Local Health Network (NALHN). The LMH serves one of the most disadvantaged urban populations in Australia10 with a substantial burden of chronic disease. As this study was designed to collect individual-level SDH data in an inpatient setting, we selected participants with three chronic diseases, which have high hospital readmission rates: diabetes mellitus, chronic obstructive pulmonary disease (COPD) and heart failure (HF).
Eligible participants were:
- ≥18–75 years
- Diagnosed with diabetes mellitus, COPD or HF
- Proficient English speakers.
Eligible participants were identified by a hospital casemix officer who provided the senior author with a daily list of all patients admitted to the LMH with a diagnosis of diabetes mellitus, COPD or HF who had been discharged from the hospital within the past 28 days. Potential participants meeting eligibility criteria were invited to participate in the study by a research team member. Informed written consent was obtained, including permission to access their medical records, and agreement to take part in a follow-up telephone interview to explore the participant’s attitudes to SDH screening. A comprehensive understanding of verbal and written English was required to provide informed consent.
Participants were asked to fill out a brief, structured paper-based questionnaire (available from: dspace.flinders.edu.au/xmlui/handle/2328/38327), which they could choose to self-complete or to complete with the assistance of a research team member. The questionnaire took approximately 10 minutes to complete and included questions in relation to education, income, employment, housing, safety and support networks. Participants who consented to take part in a follow-up semi-structured telephone interview were contacted via phone, 2–3 days after the initial screening. The phone interview was designed to take no longer than 5 minutes so it did not overburden participants, as many suffered advanced COPD and had difficulty speaking for extended periods. The follow-up interview comprised one question: “Do you think doctors should use this tool with other patients?” Responses to this question were collected and all responses were analysed to identify common themes following reflexive thematic analysis, as described by Braun and Clarke.11 Descriptive statistics were performed using IBM SPSS Statistics (Armonk, NY: IBM Corp; version 25) to explore the prevalence and type of adverse SDH present in the population. A power calculation was not performed as the primary outcome of the study was to pilot a screening tool in a specified set of hospitalised patients. A maximum sample size of 50 participants was determined to be feasible and appropriate.9
Results
Recruitment
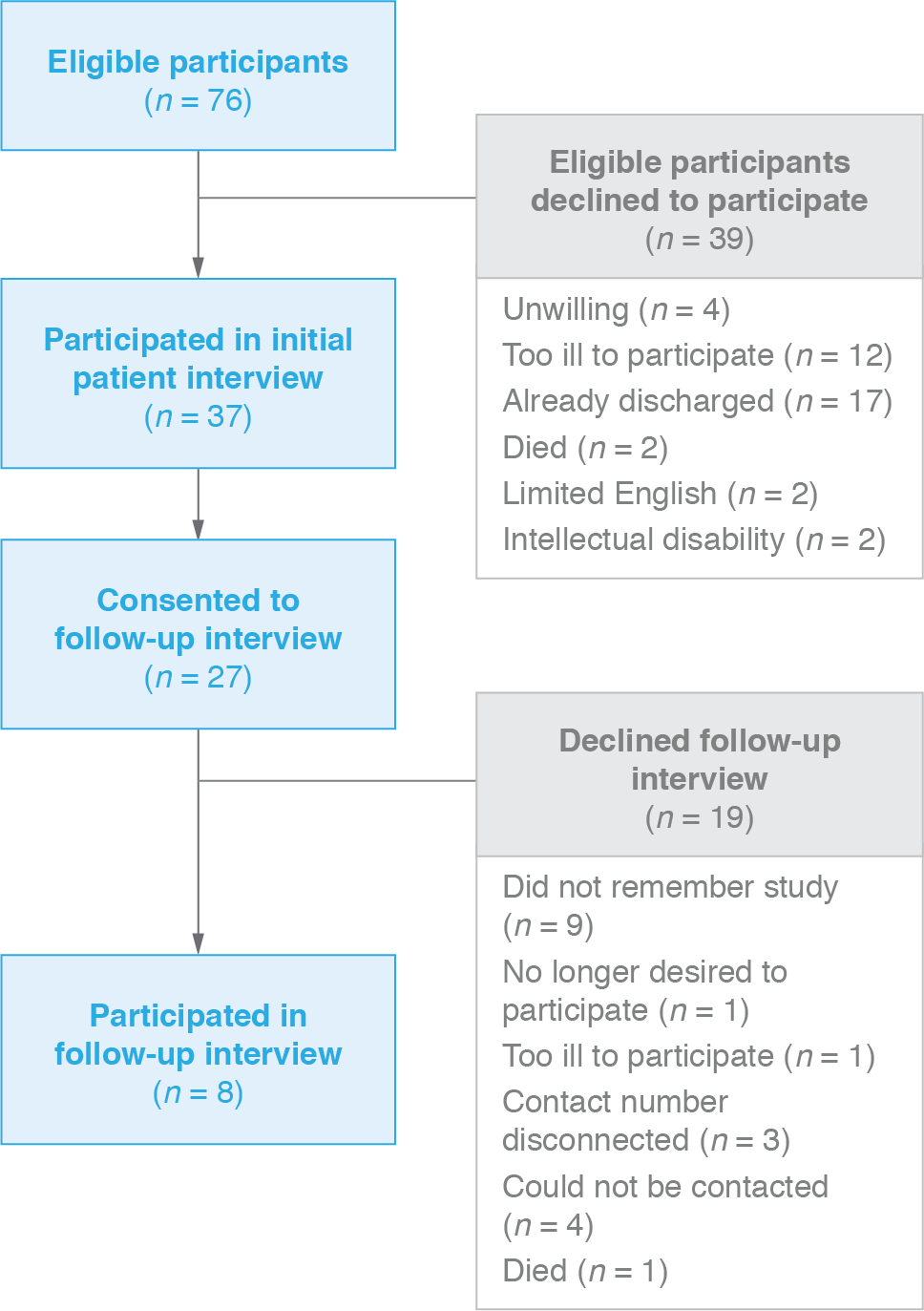
We identified 76 participants eligible for this study. Thirty-seven agreed to take part in SDH screening, of which 27 consented to a follow-up interview. Eight participants completed follow-up (Figure 1).
Figure 1. Participant flow diagram (click to enlarge)
Sociodemographics
The sample population comprised more male than female participants (Table 1). The mean age of participants was 60.3 years (standard deviation [SD] 13.9). Less than one-third of participants (32%) had completed high school, 22% possessed some high school education but not to university entrance level standard, and 19% had completed year 12. More than half the sample (57%) had received no education beyond high school, 24% attained a trade or apprenticeship, 16% possessed some form of higher education diploma, and no participants had attained a university degree. Only 11% of the sample were conventionally employed (3/37 full time, 1/37 part time); 32% reported being unable to work or receiving a disability or work cover pension and 41% fulfilled home duties or were retired. COPD was the most prevalent condition among the sample (54%), followed by HF (24%) and diabetes mellitus (22%). Some participants had multiple comorbidities, but were categorised based on the primary diagnosis that resulted in their admission to hospital. The mean number of adverse SDH reported by each participant was 4.7 (SD 2.8).
Table 1. Overview of participants’ sociodemographic characteristics and reported prevalence of adverse social determinants of health (SDH)
| Sociodemographic characteristics | Participants (N = 37) | |
| Age | Mean (standard deviation)
Median (range) |
60.3 (13.9)
62.5 (56) |
| Gender (%) | Male
Female |
22 (59)
15 (41) |
| Country of birth (n, %) | Australia
Germany Ireland New Zealand United Kingdom |
31 (84)
1 (3) 1 (3) 1 (3) 3 (8) |
| Language spoken at home (n, %) | English
Other |
37 (100)
0 (0) |
| Highest level of school education (n, %) | No formal schooling
Primary school Some high school Year 10 Year 11 Year 12 |
1 (3)
4 (11) 8 (22) 12 (32) 5 (14) 7 (19) |
| Highest qualification (n, %) | School
Trade/Apprenticeship Diploma/Associate diploma University |
22 (59)
9 (24) 6 (16) 0 (0) |
| Employment status (n, %) | Not working
Unable to work/disability/work cover Student Home duties/retired Part time/casual Full time |
6 (16)
12 (32) 0 (0) 15 (41) 1 (3) 3 (8) |
| Primary diagnosis (n, %) | Diabetes mellites
COPD HF |
8 (22)
20 (54) 9 (24) |
| Reported adverse SDH (per participant) |
Mean
Standard deviation Median |
4.7
2.8 4 |
COPD = Chronic obstructive pulmonary disease; HF = Heart failure; SDH = social determinants of health
Types of adverse social determinants of health (SDH)
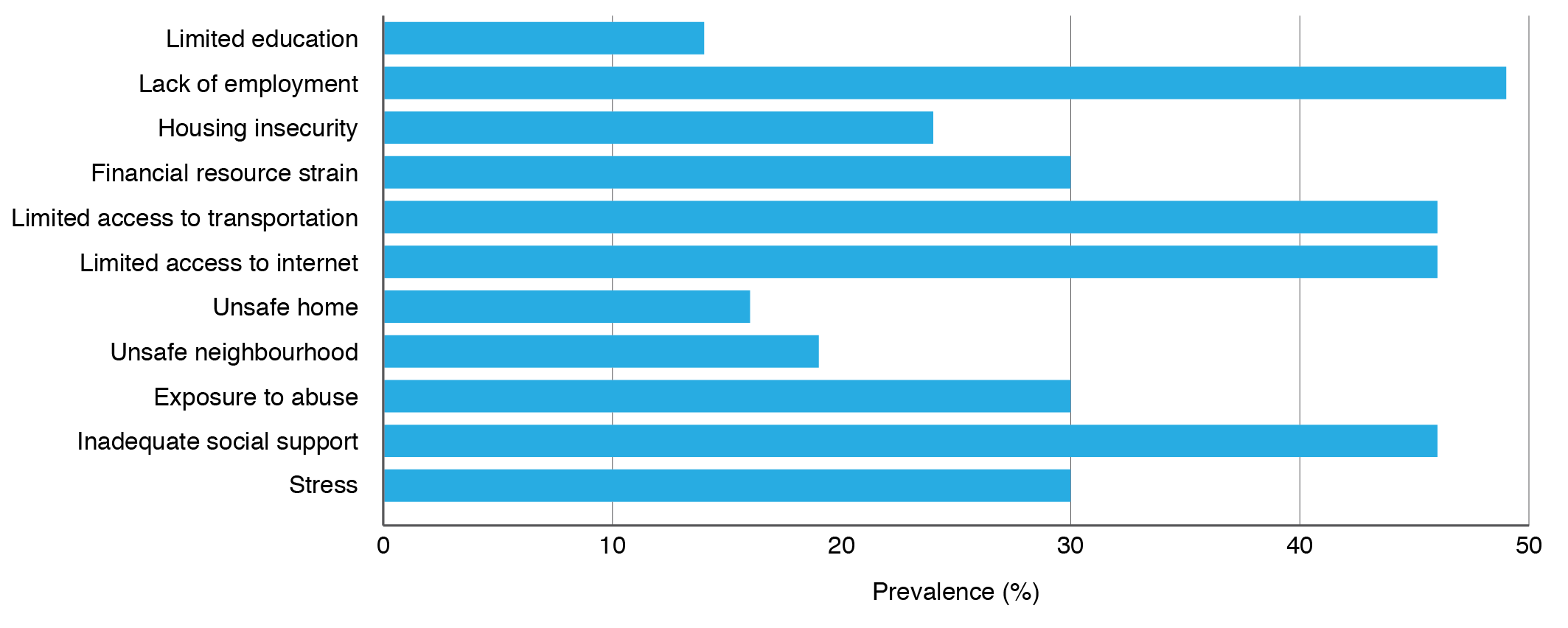
Lack of employment was the most prevalent adverse SDH reported in this population, experienced by just under half of participants (48%). Inadequate social support (46%), limited access to the internet (46%) and transportation (46%) were the second most common adverse SDH affecting this population. Stress, exposure to abuse and financial resource strain were each present in 30% of the population. Housing insecurity was reported by 24% of the population, followed by unsafe neighbourhood and home environments (19% and 16% respectively). Limited education was reported by 14% of the sample (Figure 2).
Figure 2. Prevalence of different types of adverse social determinants of health (SDH) (N = 37) (click to enlarge)
Prevalence of adverse SDH
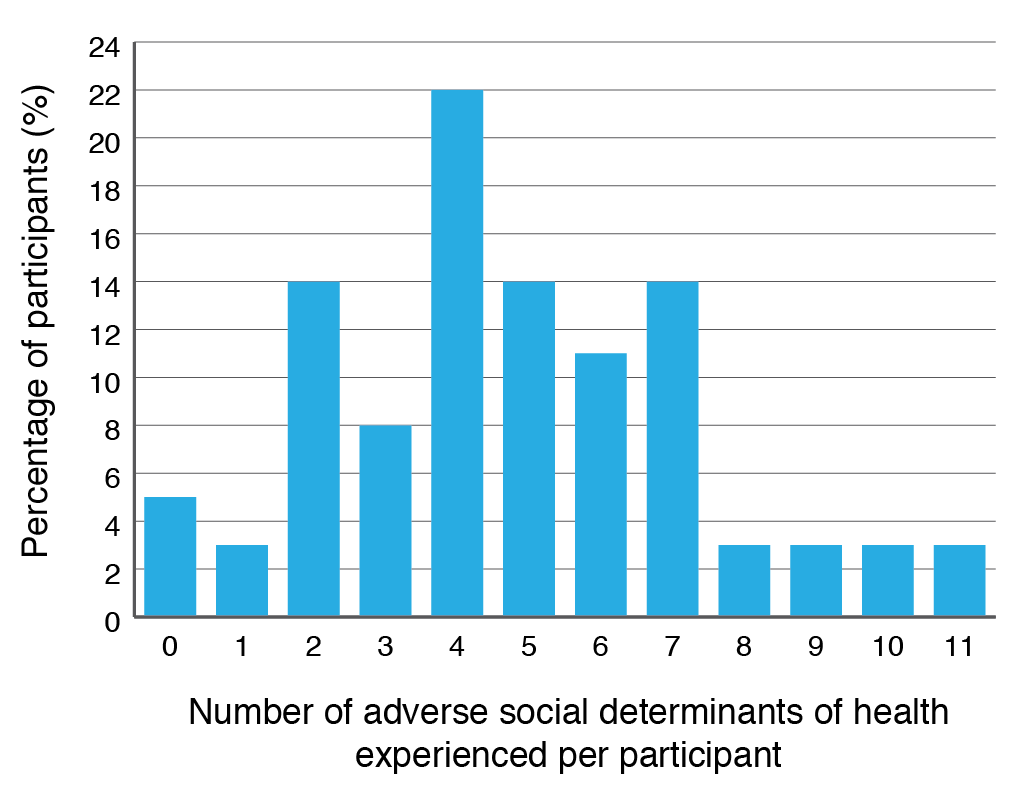
Just under one-quarter of participants (22%) reported experiencing four adverse SDH concurrently and 12% of the sample reported experiencing eight or more adverse SDH concurrently. Only 5% of participants did not report experiencing any adverse SDH (Figure 3).
Figure 3. Number of adverse social determinants of health (SDH) experienced per participant (N = 37) (click to enlarge)
Follow-up interviews
None of the participants who took part in the follow-up telephone interview (n = 8) reported any problems with understanding or reading the SDH screening tool. Seven out of eight (88%) participants believed doctors should use the same screening tool with other patients. Reflexive thematic analysis11 was applied to participants’ responses to the interview question “Do you think doctors should use this tool with other patients” and three themes were identified (Table 2). Participants believed doctors using this tool with their patients may enhance communication between healthcare providers and patients. Secondly, participants believed SDH screening may assist healthcare providers to identify underlying social problems and find different ways to help resolve these problems. Finally, participants believed conducting screening for adverse SDH would have a mixed impact on doctors. Some participants suggested SDH screening would improve patients’ health outcomes, while others suggested the extra time necessary to conduct screening would have negative impacts as doctors are already too time-poor (Table 2).
Table 2. Thematic analysis of participants’ responses to the follow-up question “Do you think doctors should use this tool with other patients?” (n = 8)
| Themes identified from question: ‘Do you think doctors should use this tool with other patients?’ | Participant responses |
| Enhance communication between healthcare provider and patient | “Yes, this helps people to talk more, writing down things is easier than talking”
“Yes, it might help learn extra what patients want” “Yes, it may help figure out healthy situations for patients and how to help them” |
| Assist to identify existing problems and new solutions | “… [The tool] may highlight any reoccurring instances where patients didn’t get the services they required. If you can’t measure it, you can’t manage it”
“Yes, it might help learn extra what patients want” “Yes, doctors should ask patients how they feel and find out what’s going on in their lives” “Yes, it may help figure out healthy situations for patients and how to help them” |
| Impact on doctors | “Maybe a researcher instead of a doctor [could conduct SDH screening], doctors are very busy, or some kind of peer worker specialist.”
“[Using the tool] would help doctors” |
Discussion
The sociodemographic composition of the sample reflected the socio-economic deprivation previously reported in the NALHN catchment area.10 In this sample, 59% of participants had received no higher education than secondary schooling and none had received tertiary education (Table 1). This finding may be partly attributed to the age of the sample (mean 60 years), as younger Australians are more likely to attend university than previous generations.12
Reported adverse SDH
Unemployment and job insecurity have serious, adverse effects on physical and mental health and wellbeing, and have been linked to increased prevalence of chronic disease.13 Less than one-third of the sample population were in paid employment, which may be due to the age of the sample (mean 60 years), although unemployment is higher in the NALHN catchment area than the average for South Australia.14 A combination of inadequate social support, lower educational attainment and limited access to transportation (Figure 1) may contribute to the prevalence of ill health in the NALHN population.15 There is evidence that inadequate social support and loneliness contribute substantially to the development of mental health and chronic illness.15 The Australian Census10 and Social Health Atlas data14 for the NALHN catchment area support our findings on financial resource strain, which might feasibly contribute to the high reported prevalence of stress and housing insecurity (Figure 2). The reported difficulty accessing the internet (Figure 1) may reflect the growing inequality in the use of and access to digital technologies.14 Evidence suggests that in Australia, people living in the most disadvantaged areas have less access to the internet than less disadvantaged populations.16
In our study, ‘exposure to abuse’ is defined as exposure to emotional, physical or financial abuse. Our small sample size means the high reported prevalence of exposure to abuse (Figure 2) may not accurately characterise the wider NALHN area. However, in Australia, certain types of abuse are reported to follow the same social gradient: the most disadvantaged populations are 1.5 times more likely to experience intimate partner violence as those living in the least disadvantaged areas.17 Our data show significant clustering of adverse SDH, with a small proportion of participants reporting 10 and 11 adverse SDH (Figure 2). This finding is representative of the reality that adverse SDH often exist in interconnected and mutually reinforcing relationships.18 The dearth of SDH research at the local community level means our findings could not be compared with other Australian populations.
Participants’ attitudes to SDH screening
Effective communication is key to improving healthcare and patient satisfaction.19 Overall, participants thought SDH screening would be effective in enabling communication between healthcare providers and patient. As one participant suggested, the tool would highlight situations where patients repeatedly failed to receive services they needed, while another said it would bring attention to factors that may not be otherwise recognised (Table 2).
Unless patients are asked whether they would prefer to write down or to discuss adverse SDH face-to-face, they may be less likely to discuss sensitive social issues with their healthcare provider. As one participant stated: “… this [the screening tool] helps people to talk more, writing down things is easier than talking” (Table 2). Currently, there is no consensus as to whether assisted or self-completion of SDH screening produces more reliable data. There is some evidence that self-administered questionnaires yield better quality data concerning highly sensitive domains, such as domestic violence and substance abuse, as the participant is likely to be less affected by social desirability bias.20 However, healthcare providers regularly cite the time necessary for conducting SDH screening as a key barrier to its implementation.8 As one participant suggested: “Maybe a researcher [should use the tool] instead of a doctor, doctors are very busy, or some kind of peer worker specialist” (Table 2). This is consistent with the finding that although patients appreciate being asked about SDH, they do not necessarily expect the healthcare system to fix these problems.21 A growing body of evidence supports employing community healthcare workers or social workers in this capacity22,23, as they are generally more experienced with SDH and referral to community resources.
To our knowledge, this pilot study was the first in Australia to capture individual-level SDH data in an inpatient setting, providing valuable insight into the nature and prevalence of social challenges facing those living in this community.
Limitations
Our study had limitations. Eligibility criteria restricted our sample to proficient English speakers; the NALHN comprises a large non-English speaking immigrant population14 who were not included, thus the adverse SDH experienced in the population may be under-reported. Participants with an intellectual disability who were unable to provide informed consent were also excluded, which may have further biased our data. The participants’ positive attitude to SDH screening may not accurately reflect the opinion of the wider population due to the small number (n = 8) who agreed to participate in the follow-up phone interview.
Conclusion
Screening of individuals for adverse SDH was conducted in a hospital serving a highly disadvantaged Australian population. The sample reported experiencing multiple adverse SDH, providing valuable insights into the social and economic challenges experienced by individuals in this community. Participants viewed SDH screening as potentially beneficial to both doctors and patients and were comfortable discussing sensitive social domains, which encourages further research into SDH in this environment. Larger studies comprising SDH screening and referral to community resources are required to improve our knowledge of how to best identify and intervene to address adverse SDH in healthcare settings.
Acknowledgements
The authors would like to acknowledge the casemix officer, medical and nursing staff at the LMH for their assistance and support during the recruitment process. The authors also thank all participants involved in the study.
Peer review and provenance
Externally peer reviewed, not commissioned.
Dedication
We dedicate this paper to our colleague Dr. Kathryn Browne-Yung in honour of her commitment to social justice. Kathryn died suddenly on 18 March 2020.
Copyright:

© 2020 Neadley et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Taylor L, Tan A, Coyle C, Ndumele C, Rogan E, Canavan M, Curry L, Bradley E. Leveraging the social determinants of health: what works?. PLoS One. 2016;11(8):e0160217. CrossRef | PubMed
- 2. Gottlieb L, Wing H, Adler N. A systematic review of interventions on patients’ social and economic needs. Am J Prev Med. 2017;53(5):719–29. CrossRef | PubMed
- 3. Bielaszka-DuVernay C. Vermont's blueprint for medical homes, community health teams, and better health at lower cost. Health Aff (Millwood). 2011;30(3):383–6. CrossRef | PubMed
- 4. Johnson D, Saavedra P, Sun E, Stageman A, Grovet D, Alfero C, et al. Community health workers and Medicaid managed care in New Mexico. J Community Health. 2012;37(3):563–71. CrossRef | PubMed
- 5. Berkowitz SA, Hulberg A, Standish S, Reznor G, Atlas SJ. Addressing unmet basic resource needs as part of chronic cardiometabolic disease management. JAMA Internal Med. 2017;177(2):244–52. CrossRef | PubMed
- 6. Askew DA, Togni SJ, Schluter PJ, Rogers L, Egert S, Potter N, et al. Investigating the feasibility, acceptability and appropriateness of outreach case management in an urban Aboriginal and Torres Strait Islander primary health care service: a mixed methods exploratory study. BMC Health Serv Res. 2016;16:178. CrossRef | PubMed
- 7. Garg A, Boynton-Jarrett R, Dworkin P. Avoiding the unintended consequences of screening for social determinants of health. JAMA. 2016;316(8):813–14. CrossRef | PubMed
- 8. Andermann, A. Screening for social determinants of health in clinical care: moving from the margins to the mainstream. Public Health Rev. 2018;39:19. CrossRef | PubMed
- 9. Browne-Yung K, Freeman T, Battersby M, McEvoy D, Baum F. Developing a screening tool to recognise social determinants of health in Australian clinical settings. Public Health Res Pract. 2019;29(4):e28341813. CrossRef | PubMed
- 10. Australian Bureau of Statistics. Census of population and housing: socioeconomic indexes for areas (SEIFA), Australia, 2016. Table 4: Statistical Area Level 1 (SA1) Index of Economic Resources 2016. Canberra: ABS; 2018 Mar 27 [cited 2020 May 6]. Available from: www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/2033.0.55.0012016?OpenDocument
- 11. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. CrossRef
- 12. Australian Bureau of Statistics. Census of population and housing: reflecting Australia – stories from the census, 2016. Canberra: ABS; 2017 Oct 23 [cited 2020 May 6]. Available from: www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/2071.0~2016~Main%20Features~Educational%20Qualifications%20Data%20Summary%20~65
- 13. Nie J, Wang J, Aune D, Huang W, Xiao D, Wang Y et al. Association between employment status and risk of all-cause and cause-specific mortality: a population-based prospective cohort study. J Epidemiol Community Health. 2020;74:428–36. CrossRef | PubMed
- 14. Public Health Information Development Unit. Social health atlas of Australia: South Australia; 2017 Sep. South Australia: PHIDU; 2017 [cited 2020 May 5]. Available from: phidu.torrens.edu.au/social-health-atlases/data#social-health-atlas-of-australia-population-health-areas
- 15. Institute of Medicine. Capturing social and behavioral domains and measures in electronic health records: Phase 2. Washington, DC: The National Academies Press; 2014 [cited 2020 May 6]. Available from: www.ncbi.nlm.nih.gov/books/NBK268995/pdf/Bookshelf_NBK268995.pdf
- 16. Baum F, Newman L, Biedrzycki K. Vicious cycles: digital technologies and determinants of health in Australia. Health Promot Int. 2014;29(2):349–60. CrossRef | PubMed
- 17. Australian Institute of Health and Welfare. Family, domestic and sexual violence in Australia: continuing the national story 2019: in brief. Canberra: AIHW; 2019 Jun 5 [cited 2020 May 6]. Available from: www.aihw.gov.au/reports/domestic-violence/family-domestic-and-sexual-violence-in-australia-c/contents/table-of-contents
- 18. Braveman P, Egerter S, Williams D. The social determinants of health: coming of age. Annu Rev Public Health. 2011;32:381–98. CrossRef | PubMed
- 19. Burgener A. Enhancing communication to improve patient safety and to increase patient satisfaction. The Health Care Manager. 2017;36(3):238–43. CrossRef | PubMed
- 20. Gottlieb L, Hessler D, Long D, Amaya A, Adler N. A randomized trial on screening for social determinants of health: the iScreen study. Pediatrics. 2014;134(6):e1611–8. CrossRef | PubMed
- 21. Byhoff E, De Marchis EH, Hessler D, Fichtenberg C, Adler A, Cohen AJ, et al. Part II: a qualitative study of social risk screening acceptability in patients and caregivers. Am J Prev Med. 2019;57(6S1):S38–46. CrossRef | PubMed
- 22. Page-Reeves J, Kaufman W, Bleecker M, Norris J, McCalmont K, Ianakieva V, et al. Addressing social determinants of health in a clinic setting: the WellRx pilot in Albuquerque, New Mexico. J Am Board Fam Med. 2016;29(3):414–8. CrossRef | PubMed
- 23. Garg A, Toy S, Tripodis Y, Silverstein M, Freeman E. Addressing social determinants of health at well child care visits: a cluster RCT. Pediatrics. 2015;135(2):e296–304. CrossRef | PubMed