Abstract
Objective and importance of study: The importance of social determinants for individual health recovery outcomes is well recognised in public health. However, no succinct social health screening (SHS) tool exists that has been developed with information from clinicians and patients. This proof-of-concept study asked health consumer advocates, patients and clinicians about their attitudes towards social determinants of health (SDH) and the usefulness of an SHS tool for collecting these data for use in clinical settings. We then developed a streamlined SHS tool to bring this knowledge to clinicians, and conducted a proof-of-concept trial to check its acceptability with patients and clinicians.
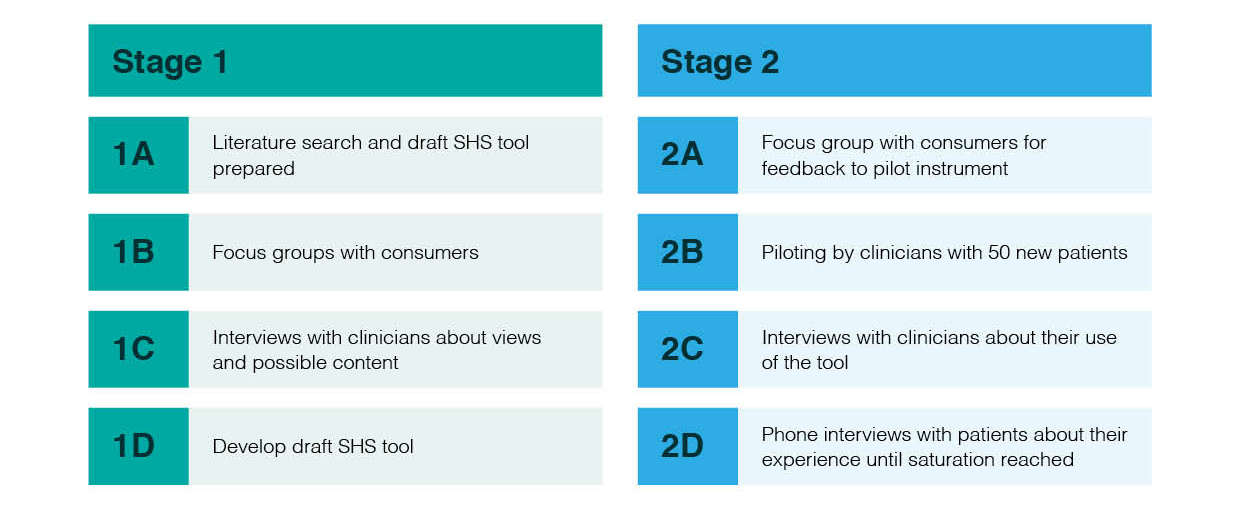
Methods: This qualitative study had two stages. Stage 1 involved focus groups with health consumer advocates and interviews with clinicians about the draft SHS tool. Stage 2 involved refining the SHS tool and piloting it with 50 new patients in anxiety disorder and sleep disorder clinics, which often treat patients living in disadvantaged socio-economic conditions. The tool was evaluated by patients and clinicians. The data were analysed using framework analysis.
Results: All interviewees were positive about the benefits of addressing SDH in clinical practice to help reduce health inequities. We developed and refined an SHS tool that could be completed by patients (‘self-complete’).
Conclusion: The response to introducing an SHS tool in clinical settings was positive. Further piloting across diverse clinical settings is required to determine efficacy. This tool promotes public health equity outcomes by improving clinician understanding of individual social circumstances, and has the potential to provide useful epidemiological data on SDH.
Full text
Introduction
Individuals experiencing adverse social determinants of health (SDH) are more likely to have poorer health outcomes than those with advantageous social determinants.1 In Australia, socio-economically disadvantaged groups generally have a lower life expectancy and a higher risk of chronic disease.2 Acknowledging a patient’s social circumstances – such as access to transportation, and their housing and economic situation – in clinical settings may significantly influence the effectiveness of healthcare outcomes for that patient.3 Information about patients’ social and economic living conditions is not routinely collected in clinical settings, but could help clinicians to contextualise patient care. Such information may sometimes be available to clinicians but it is not routinely or systematically collected.
Allen et al. argue that clinicians often underuse opportunities to improve their patients’ SDH.1 They recommend routinely taking a patient’s social history together with a medical history. Introducing a social health screening (SHS) tool would give clinicians information about constraints that some patients experience in their lives, including unemployment, low income and insecure housing. It would also give clinicians a better understanding of potential reasons for noncompliance with clinical advice, and inform them about general adversities in patients’ lives that affect how they experience illness.4 Research, population health and health service planning would benefit from integrating information from the tool into electronic data collection systems. The data would support examination of the detailed ways in which SDH affect health equity, and people’s access to and effective use of health services.3
Barriers and facilitators to using SHS tools in clinical settings include time, cost, reluctance to ask about ‘taboo’ topics such as domestic violence, and clinicians’ unfamiliarity with hardship in their patients’ lives.5,6 Beck et al.5 suggest that further research is needed to determine what would encourage clinicians to ask sensitive questions. Suggested explanations for clinicians’ reluctance to engage in these conversations with patients include a sense of powerlessness in being able to address the root causes underlying difficult circumstances, or feeling that the causes are beyond the scope of health services to help.3,7
However, increased interest in the effects of social factors on patient care and recovery has seen rapid growth in SDH interventions integrated into electronic healthcare delivery systems, particularly in North America. A recent review identified 67 tools that include questions about one or more SDH, including legal aid, education, literacy levels and food security.8 Other studies identified SHS tools used in Europe and New Zealand.5,9-17 The studies reinforced the importance of developing social history tools and recognised the importance of information about SDH to good clinical practice. No tool was sufficiently brief to allow patients to complete the questions while waiting for clinical appointments. A focus on specific SDH and particular groups made some tools unsuitable for a wide range of clinical settings because some questions would be irrelevant. For example, the DiPCare-Q16,17 is not self-complete, the PQoL18 includes items specific to particular cultural settings, and the NZiDep14 refers exclusively to material disadvantage. None of these studies included clinician and patient attitudes to SDH, or the acceptability of SDH tools or their usefulness during clinical appointments.
This study sought to fill the research gap by determining the views of clinicians and health consumer advocates on SHS tools and their usefulness. Based on this information, we developed a brief self-complete SHS tool that would inform clinicians about social determinants in their patients’ lives that could be discussed in more detail during consultations. This proof-of-concept study was conducted in anxiety and sleep disorder clinics, which often treat patients with conditions that have underlying inequity issues. The social inequality risk factors for mental illness include low income, unemployment, low social capital and social exclusion.19 In addition, poorly managed physical chronic disease is partly responsible for the 10–15-year lower life expectancy of people with severe mental illness compared with the general population.20 A major risk factor for obstructive sleep apnoea (OSA) is obesity, which has also been linked to socio-economic disadvantage.21 OSA incidence has increased from around 3% to 16% since the mid-1990s.22 The following section describes the development and piloting of the SHS tool. This study was approved by the Southern Adelaide Clinical Human Research Ethics Committee (578.13 – HREC/13/SAC/419).
Methods
The methods are summarised in Figure 1.
Figure 1. Developing the Social Health Screening (SHS) tool (click to enlarge)
Stage 1
In Stage 1 we developed the draft tool using items from existing instruments and theoretical frameworks5,23-25 and from the research group’s expertise in SDH. The criteria for inclusion were that domains reflected the social and material conditions of living that potentially affect a patient’s ability to comply with treatment, which would affect recovery. The initial stage included focus groups with three females and three males recruited from an independent volunteer health consumer group, all of whom had consumer experience of health services and most of whom were retired allied health professionals. Focus groups create an environment of collaboration and allow for consensus to develop through the collaborative process of constructing a joint perspective and agreement.26 The focus groups examined health service users’ attitudes and orientation towards using an SHS tool in clinical settings. They were moderated by the second author, with the first author acting as observer and note-taker. Participants were compensated for their time with a $35 gift voucher.
Individual interviews (n = 16) were held with a range of clinicians including doctors, nurses and psychologists from two clinics: one for anxiety disorder conditions and the other for sleep health. The third and fourth authors (a psychiatrist and a physician) are directors of the respective clinics, and the first author (unaffiliated to either clinic) carried out the interviews. In addition to the topics covered in Appendix 1 (see supplementary material, available from: hdl.handle.net/2328/38327) the first author asked clinicians to state specific information about SDH that they would find useful. Items for inclusion were further developed during regular research team meetings based on the data collected in focus groups and interviews.
Stage 2
Based on the outcomes of Stage 1, we refined the draft SHS tool. We held an additional health consumer focus group (three females and two males), using the same recruitment methodology. The focus group determined the appropriateness of the questionnaire length, wording of questions, response options, and face and content validity before piloting.
The draft self-complete questionnaire (see supplementary material, available from: hdl.handle.net/2328/38327) was then piloted with 50 new patients (25 from each clinic). The first author approached new clinic patients, explained the project and obtained written consent. Consenting patients completed the questionnaire before their first clinical consultation and gave verbal feedback to the researcher about its content, wording and language, degree of difficulty, and time needed to complete. Patients were asked if they were willing to participate in a follow-up telephone call to answer questions about their consultation experience using the SHS tool, and received a $35 gift voucher for their time.
Twelve clinicians reviewed the information on the tool before seeing new patients. After the consultation, each clinician completed a brief feedback questionnaire on use and content validity. When 50 patients had completed the tool, the first and second authors undertook audio-recorded interviews with six clinicians to determine the perceived barriers and facilitators to using the tool, and whether the tool was beneficial to clinicians in approaching sensitive issues.
The interview transcripts and focus group data were checked and initial coding performed based on the SDH and SHS tool topics covered. Using framework analysis through familiarisation, indexing, charting, mapping and interpretation of the data, the codes were further expanded and references to SDH and key topics for inclusion were identified.27 We created a coding framework and identified the emergent SDH themes. Focus groups were attended by both the first and second authors who took detailed notes on health consumer feedback and the issues raised. Their notes were compared and coded for emergent themes. All the themes identified were used to guide the development of the SHS tool.
Results
Focus group and clinician input
Both the focus groups and the clinicians were positive about the use of an SHS tool and viewed it as a conversation starter with patients. A common approach repeated by clinicians was that occupation and subjective visual cues (such as dress) were often relied on as proxies for a patient’s financial situation, and additional information would be useful. Clinicians acknowledged there was no systematic way of collecting such data. Key issues raised about the tool included legibility, length and the need for a broad question probing abuse.
Focus group members noted the following:
- A streamlined SHS tool designed for clinicians to start a conversation about social issues that may affect health and recovery was viewed positively, and there was a need for it
- There is variation in literacy levels and language fluency, so the questionnaire should aim for primary school reading level
- Some patients may need help completing the questionnaire
- Patients get tired of filling out the same information in numerous forms, so there is a need to avoid duplication.
Clinicians noted the following:
- Some of the information was already gathered in disparate ways in both clinics, but having a brief consolidated tool would save time and be useful in settings where this information is not collected
- A streamlined SHS tool would save time
- The tool would be useful because they may get this information during several consultations but there is no systematic approach in place
- The tool should be brief, simple and self-complete; it should definitely not be completed face-to-face with clinicians as they are too busy
- It is important to know about social issues (such as transport) and financial issues for ongoing compliance with treatment; this information would signpost potential problems
- The overall language is easy to understand and read and the questions are well grouped
- Knowing whether a patient has internet access is important because patients often search for medical knowledge there first
- The patient’s family and level of network support is very important to include.
We made the following changes in response to this feedback:
- Included transgender in the gender question
- Simplified the wording to allow for low literacy levels (e.g. ‘precarious housing’ was changed to ‘at risk of losing your home’)
- Introduced emojis in questions 20 and 25 for visual representation
- Removed ‘terrace house’ from housing type and included ‘caravan or mobile home’
- Added ‘retirement village’ to options and cut down ‘to own or rent’
- Added questions to capture emotional, physical and financial abuse
- Condensed the tool into four pages
- Added an opportunity for comment at the end
- Removed duplicated demographic information.
Proof-of-concept trial
The tool took 6 minutes to complete, on average. All were self-completed. The questions were considered easy to read and not too sensitive. All 50 participants said they would be comfortable completing the tool in other clinical settings. Telephone interviews were undertaken with five patients, which reinforced previous feedback. The following is a typical response:
Fine, no worries. Nothing majorly personal. It was easy to understand and straightforward. (Male patient, anxiety disorders clinic)
None of those interviewed had noticed whether the clinician had used the information they provided and were unsure whether it had affected their first consultation. The small sample size did not include any patients with adverse SDH. Similar to the immediate feedback after completing the tool, some participants acknowledged that they might have felt less comfortable filling out the tool if they had experienced some of the issues explored, such as precarious housing or domestic violence. Twelve clinicians from both clinical settings participated in the proof-of-concept trial. The key responses are shown in Box 1.
Box 1. Key open-ended responses from clinicians after using the SHS tool
- Recommend this information be collected. Don’t want to collect duplicate information. Form would need to be reconciled with what is already systematically collected on other forms
- Lengthened the consultation, would be good if not already collecting this information – collecting very similar info
- Might be useful in certain circumstances, busy GP practice or emergency departments
- Did not influence care with this patient or lengthen consultation. Would need to use on more patients to get idea of how useful it is
- First consultations can be more than 1 hour
- Other measures more useful; we also do a full psychosocial screening, which provides more information. May be more appropriate in other areas where full history is not done
- Reduced consultation time
- Useful, as was able to get a feel for the client’s level of depression/mood – not anxiety; it allowed me to feel comfortable knowing that the client had support people around her
- Was useful for reference when questioning the client. Helped plan session especially around mood. Could start assessing this having some prior knowledge
- We also obtain similar information – may be useful for places with no means to obtain this info
- Would be good if information wasn’t already available.
Overall, the feedback from clinicians was positive, and all recommended using the tool in clinical settings, especially with patients they are seeing for the first time. The clinicians also said the tool would be useful in emergency departments and busy general practices where a rapid overview is required. Patients identified as having adverse SDH could be given appropriate support and treatment tailored to their circumstances, to increase the likelihood that treatment will be effective and patients will comply with therapies.
Limitations
Both clinics used in this study had existing mail-out assessment tools that collected SDH data from new patients, which may have affected our ability to assess the efficacy of the SHS tool. The anxiety disorders clinic tool included patient social history questions about general distress (Kessler 10), occupation and social support. The sleep clinic tool included questions on occupation and employment. Another limitation was that the small sample size did not include patients with adverse SDH.
Discussion
There is growing recognition of the importance of patients’ SDH information to good clinical practice.1 However, only a small number of brief self-complete SHS tools exist, and none of these can be easily adapted for universal clinical settings. The streamlined self-complete SHS tool developed in this study captured the key social determinants that influence health and wellbeing. It could be used by clinicians to start a dialogue with patients about their individual needs, and to aid compliance with treatment and recovery.3
The tool was easy and efficient to use. The self-complete nature of the tool allowed patients to disclose topics that may be raised in the consultation. All the clinicians involved stated that the SHS tool would be useful in clinics where SDH information is unavailable.
The contradictory response findings, where clinicians were positive about the tool but reported not using the tool in their consultation, can be explained by the small sample size not having reported any adverse social issues. This shows that the clinicians read the patient responses to determine this.
During telephone interviews, patients reported being unaware whether their clinician had used the tool. This uncertainty needs to be addressed to avoid patients feeling that they are providing information unnecessarily. We would recommend for future use that clinicians acknowledge to the patient that they have read the tool. Clinicians did not report feeling uncomfortable broaching sensitive topics, but previous literature suggests they might.5 We suggest that training for clinicians about use of the tool, and how to ask about the social conditions of patients’ lives, would maximise the tool’s effectiveness.
Routinely collected de-identified data could potentially be useful epidemiological data to examine interactions between health service use and SDH. Such data would also be helpful to determine which social determinants affect the likelihood of readmission to hospital, as well as frequent use of health services. The SHS tool promises to be particularly useful when clinicians see a patient for the first time, such as in an oncology clinic or emergency department. The tool requires piloting with a larger sample in different clinical settings, with individuals from different backgrounds experiencing adverse SDH, to ascertain its effectiveness.
Conclusion
Clinicians are aware that social and economic circumstances have a profound impact on a patient’s ability to access health services, and to manage health conditions and outcomes. This proof-of-concept study of an SHS tool is the first stage in helping identify patient social determinants for clinical and public health use. We would recommend piloting the tool in busy clinical settings where people presenting for first clinical consultation are more likely to experience a range of socio-economic disadvantage.
Acknowledgements
This project was supported by a Flinders University Faculty of Health Sciences seeding grant of $16 000 for 2013–14.
Peer review and provenance
Externally peer reviewed, not commissioned.
Copyright:

© 2018 Browne-Yung et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Allen M, Allen J, Hogarth S, Marmot M. Working for health equity: the role of health professionals. London: UCL Institute of Health Equity; 2013 [cited 2018 Mar 3]. Available from: www.instituteofhealthequity.org/resources-reports/working-for-health-equity-the-role-of-health-professionals/
- 2. Australian Institute of Health and Welfare. Australia’s Health 2016. Canberra: AIHW; 2016 [cited 2018 Mar 3]. Available from: www.aihw.gov.au/getmedia/9844cefb-7745-4dd8-9ee2-f4d1c3d6a727/19787-AH16.pdf.aspx?inline=true
- 3. DeVoe JE, Bazemore AW, Cottrell EK, Likumahuwa-Ackman S, Grandmont J, Spach N, et al. Perspectives in primary care: a conceptual framework and path for integrating social determinants of health into primary care practice. Ann Fam Med. 2016;14(2):104–8. CrossRef | PubMed
- 4. Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving chronic illness care: translating evidence into action. Health Aff (Millwood). 2001;20(6):64–78. CrossRef | PubMed
- 5. Beck AF, Klein MD, Kahn RS. Identifying social risk via a clinical social history embedded in the electronic health record. Clin Pediatr (Phila). 2012;51(10):972–7. CrossRef | PubMed
- 6. O'Toole JK, Burkhardt MC, Solan LG, Vaughn L, Klein MD. Resident confidence addressing social history: is it influenced by availability of social and legal resources? Clin Pediatr (Phila). 2012;51(7):625–31. CrossRef | PubMed
- 7. Behforouz HL, Drain PK, Rhatigan JJ. Rethinking the social history. N Engl J Med. 2014;371(14):1277–9. CrossRef | PubMed
- 8. Gottlieb LM, Wing H, Adler NE. A systematic review of interventions on patients’ social and economic needs. Am J Prev Med. 2017;53(5):719–29. CrossRef | PubMed
- 9. Carey B, Stassen L. An audit comparing the discrepancies between a verbal enquiry, a written history, and an electronic medical history questionnaire: a suggested medical history/social history form for clinical practice. J Ir Dent Assoc. 2010;57(1):54–9. PubMed
- 10. Chen ES, Manaktala S, Sarkar IN, Melton GB. A multi-site content analysis of social history information in clinical notes. AMIA Annu Symp Proc. 2011;2011:227–36. PubMed
- 11. Pierce MC, Kaczor K, Thompson R. Bringing back the social history. Pediatr Clin North Am. 2014;61(5):889–905. CrossRef | PubMed
- 12. Melton GB, Manaktala S, Sarkar IN, Chen ES. Social and behavioral history information in public health datasets. AMIA Annu Symp Proc. 2012;2012:625–34. PubMed
- 13. Eroğlu S. Developing an index of deprivation which integrates objective and subjective dimensions: extending the work of Townsend, Mack and Lansley, and Halleröd. Soc Indic Res. 2007;80(3):493–510. CrossRef
- 14. Salmond C, Crampton P, King P, Waldegrave C. NZiDep: A New Zealand index of socioeconomic deprivation for individuals. Soc Sci Med. 2006;62(6):1474–85. CrossRef | PubMed
- 15. Sass C, Gueguen R, Moulin J, Abric L, Dauphinot V, Dupre C, et al. Comparison of the individual deprivation index of the French Health Examination Centres and the administrative definition of deprivation. Sante publique (Vandoeuvre-les-Nancy, France). 2006;18(4):513–22. CrossRef
- 16. Vaucher P, Bischoff T, Diserens E-A, Herzig L, Meystre-Agustoni G, Panese F, et al. Detecting and measuring deprivation in primary care: development, reliability and validity of a self-reported questionnaire: the DiPCare-Q. BMJ Open. 2012;2(1):e000692. CrossRef | PubMed
- 17. Bodenmann P, Favrat B, Wolff H, Guessous I, Panese F, Herzig L, et al. Screening primary-care patients forgoing health care for economic reasons. PLoS One. 2014;9(4):e94006. CrossRef | PubMed
- 18. Boyer L, Baumstarck K, Iordanova T, Fernandez J, Jean P, Auquier P. A poverty-related quality of life questionnaire can help to detect health inequalities in emergency departments. J Clin Epidemiol. 2014;67(3):285–95. CrossRef | PubMed
- 19. Friedli L. Mental health, resilience and inequalities. Copenhagen: World Health Organization; 2009 [cited 2017 Sep 1]. Available from: www.euro.who.int/document/e92227.pdf
- 20. Goff DC, Sullivan LM, McEvoy JP, Meyer JM, Nasrallah HA, Daumit GL, et al. A comparison of ten-year cardiac risk estimates in schizophrenia patients from the CATIE study and matched controls. Schizophr Res. 2005;80(1):45–53. CrossRef | PubMed
- 21. Devaux M, Sassi F. Social inequalities in obesity and overweight in 11 OECD countries. Eur J Pub Health. 2012;23(3):464–9. CrossRef | PubMed
- 22. Choudhury S, Taheri S. Obstructive sleep apnoea and type 2 diabetes: whose disease is it anyway? Pract Diabetes Int. 2011;28(4):183–6a. CrossRef
- 23. Marmot M. Social determinants of health inequalities. Lancet. 2005;365(9464):1099–104. PubMed
- 24. Dahlgren G, Whitehead M. Policies and strategies to promote equity in health. Stockholm: Institute for Futures Studies; 1991 [cited 2018 Feb 2]. Available from: www.researchgate.net/profile/Goeran_Dahlgren/publication/5095964_Policies_and_strategies_to_promote_social_equity_in_health_Background_document_to_WHO_-_Strategy_paper_for_Europe/links/569540f808aeab58a9a4d946.pdf
- 25. Elo A-L, Leppänen A, Jahkola A. Validity of a single-item measure of stress symptoms. Scand J Work Environ Health. 2003;29(6):444–51. CrossRef
- 26. Smithson J. Using and analysing focus groups: limitations and possibilities. Int J Soc Res Methodol. 2000;3(2):103–19. CrossRef
- 27. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Huberman MA, Miles MB, editors. The qualitative researcher’s companion. Thousand Oaks, CA: Sage Publications; 2002.