Abstract
Objectives: To analyse trends in smoking initiation and prevalence among young Aboriginal and Torres Strait Islander people (Indigenous people) to identify which stages of adolescence and young adulthood prevention activities should target.
Methods: Secondary analysis of ‘daily smoking’ and ‘never smoked’ responses from Indigenous people aged 15 years and older in five national Indigenous surveys from 2002 to 2014–15, and of initiation age among those aged 18 years and older in 2004–05 and 2012–13.
Results: Smoking prevalence among 15–24-year-olds declined significantly between 2002 and 2014–15, falling 14 percentage points (95% confidence interval [CI] 8, 21) from 45% to 31%. The greatest decline was among 18–19-year-olds, with a decrease of 17 percentage points (95% CI 4, 29) from 48% to 31%. The proportion of 15–24-year-olds who had never smoked increased significantly, by 12 percentage points (95% CI 6, 18) from 44% in 2002 to 56% in 2014–15.
Between 2004–05 and 2012–13, the proportion of 18–24-year-old smokers who had started daily smoking before the age of 18 years declined significantly, down 8 percentage points (95% CI 2, 15) from 84% to 76%. In 2012–13, 24% of smokers aged 18–24 years started daily smoking after age 18, half (49%) started between 15 and 18 years, and around a quarter started before age 15.
Conclusions: There have been significant declines in smoking prevalence among young Indigenous people between 2002 and 2014–15 as fewer take up smoking. Smoking initiation occurs over a wide age range. The majority of daily smokers started before the age of 18; however, initiation may be delayed until early adulthood for an increasing number. The challenge for tobacco prevention is to reach young people in early adolescence and continue to reinforce smoke-free intentions into young adulthood.
Full text
Introduction
Tobacco use continues to be a major cause of preventable ill health for Aboriginal and Torres Strait Islander people (Indigenous people), contributing to deaths and disability from cancer, and respiratory and cardiovascular diseases. Smoking is the largest contributing risk factor (23%) to the gap in disease burden between Indigenous people and non-Indigenous Australians1, a legacy of the social and economic impacts of colonisation and a disparity shared with other populations with a similar historical context (New Zealand, Canada and the US).2
Although the most recent national data showed current smoking among Indigenous people to be 2.7 times higher than among non-Indigenous people3,4, there have been positive improvements over the past two decades, with a significant decline in adult smoking rates from 55% in 1994 to 45% in 2014–15.5
Reducing smoking prevalence involves supporting existing smokers to quit and preventing smoking initiation. Most regular smoking begins during adolescence and young adulthood, defined in this paper as 10–24 years: early adolescence (10–14), late adolescence (15–19) and young adulthood (20–24).6 Almost all (99%) daily smokers begin smoking before age 26.7 Promisingly, the greatest declines between 2002 and 2014–15 were recorded in the 15–17 and 18–24 years age groups, down from 33% to 17% and 58% to 41%, respectively.4 There was also an increase in young ‘never-smokers’ over the same period, indicating fewer young people are taking up smoking.3,4
Smoking uptake involves transitioning through different stages that may occur over several years, beginning with the first try (a few puffs to a full cigarette), then repeated experimentation, before establishing regular smoking (consumed 100 cigarettes and/or at least daily smoking for more than 1 month).8,9 Smoking prevention can target any or all of these stages.10 Many young people do not progress beyond experimentation, and, for those who do, the timing of these transitions is not uniform. One model of initiation describes four trajectories: ‘early establishers’ (trying cigarettes at around 12–13 years of age, progressing to daily use by age 17); ‘late establishers’ (beginning around 15–16 years of age, with use peaking in the early 20s); ‘quitters’ (who experiment early, before 11 years of age, and peak at less than daily use at age 16); and ‘nonsmokers’.7
Population health surveys measuring smoking uptake differ in the stage reported: some record the age of the first full cigarette smoked, others the age daily smoking commenced. The 2016 National Drug Strategy Household Survey (NDSHS) found that the mean age of first smoking a full cigarette for all Australian youth has increased significantly over time from 14 years in 1995 to 16 years in 2016.11 The most recent NDSHS data reporting the age of the first full cigarette smoked for young Indigenous people are from 2013. The data showed no significant changes between 2010 and 2013, with the first full cigarette smoked at around 15 years of age.12 However, the NDSHS does not record the age that regular smoking commenced, and includes few survey participants from remote areas. This is a significant limitation of this dataset given that, at the 2011 census, 21% of Indigenous people were recorded as living in remote regions13, where smoking prevalence is also known to be higher than in other areas.3,14
In contrast, cross-sectional surveys by the Australian Bureau of Statistics (ABS) – National Aboriginal and Torres Strait Islander Health Survey (NATSIHS), Australian Aboriginal and Torres Strait Islander Health Survey (AATSIHS) and National Aboriginal and Torres Strait Islander Social Survey (NATSISS) – reflect the geographic distribution of the Aboriginal population, including in remote areas. The health surveys also record the age that daily smoking commenced. Data from a recent analysis of smoking trends among Indigenous people who had ever smoked daily showed that the proportions of people aged 18 years or older who started smoking before age 18 years were similar over time: 70% in 2004–05 and 69% in 2012–13.5 This analysis also found an overall decrease of 13 percentage points in the prevalence of current smoking among 15–17-year-olds, from 30% in 1994 to 17% in 2014–15, and an average annual relative decrease of 4%, indicating a reduction in smoking uptake.5
However, analysis of clinic data from Victorian Aboriginal Community Controlled Health Organisation (VACCHO) member services suggests higher smoking prevalence among 20–24-year-olds than 15–19-year-olds, which may indicate that the improvements in teenage smoking could be due to more young people delaying smoking initiation until their 20s.
This paper extends previous national analyses of smoking initiation trends by investigating smoking prevalence among 15–24-year-olds, and the age at which 18–24-year-old smokers and ex-smokers started to smoke. It is part of a broader project led by VACCHO.
Methods
Data sources
Data sources were the 2002, 2008 and 2014–15 NATSISS, the 2004–05 NATSIHS and 2012–13 AATSIHS, collected between August 2002 and April 2003, August 2004 and July 2005, August 2008 and April 2009, April 2012 and February 2013, and September 2014 and June 2015. There were 9359 (2002), 5757 (2004–05), 7823 (2008), 6037 (2012–13) and 7022 (2014–15) Indigenous respondents aged 15 years and older (18 years and older for the 2004–05 NATSIHS).
Data collection methods and access
Data collection for the ABS surveys included face-to-face interviews of a multistage random sample of Indigenous people identified as usual household residents of private dwellings. Further details are available in the ABS technical user guides.15-19
Data were obtained from confidentialised unit record files for the 2002, 2008, 2014–15 NATSISS, 2004–05 NATSIHS and 2012–13 AATSIHS, accessed through the ABS Remote Access Data Laboratory.
Outcome and predictor variables
Outcome variables included smoking status (daily and never smoking) from each survey from 2002 to 2014–15, and age daily smoking commenced from the 2004–05 NATSIHS and 2012–13 AATSIHS. Daily smoking (and age it commenced) was defined as at least one cigarette a day. See Supplementary Table 1 (available from: doi.org/10.26188/5c99c4be884cb) for question variations. Never-smokers were defined differently in the NATSISS (never smoked daily) and the NATSIHS/AATSIHS (less than 100 cigarettes in a lifetime or other tobacco products less than 20 times).
Predictor variables included age, gender, state or territory, and remote/non-remote location.
Data analysis
Estimates of smoking prevalence, never-smoked status and the age daily smoking commenced were obtained from all surveys using Stata 10 (College Station, TX: StataCorp LP; special edition). Weighted population estimates and standard errors were calculated using reference weights as described by Donath20, and the variances of the differences between estimates were calculated from the sum of the variances of the estimates.
Results are for Indigenous people nationally, with subgroup analyses by gender, remoteness, age group and state/territory (excluding Tasmania and the Australian Capital Territory, which are combined by the ABS in several surveys).
Daily smoking and never-smoked status were compared between the 2002 NATSISS and subsequent surveys for groups within the 15–24 age range (18–24 in 2004–05, when smoking data were restricted to those aged 18 or older).
Due to the age limits in 2004–05, comparisons between surveys in age of smoking initiation are for those aged 18 or older. Comparisons were also made within and between the 2004–05 and 2012–13 surveys across 10-year age groups (20–29, 30–39, 40–49, 50 years and older) to determine whether any changes are due to a longer-term cohort effect. The nearly 10-year gap between surveys means most current and ex-smokers would have moved into the next 10-year age group; for example, 40–49-year-olds surveyed in 2012–13 would be from the same birth cohort as 30–39-year-olds surveyed in 2004–2005.
Ethics approval
The Menzies School of Health Research and the Northern Territory Department of Health Top End Human Research Ethics Committee Indigenous subcommittee provided ethics approval (HREC-2012-1844).
Results
Changes in daily smoking prevalence
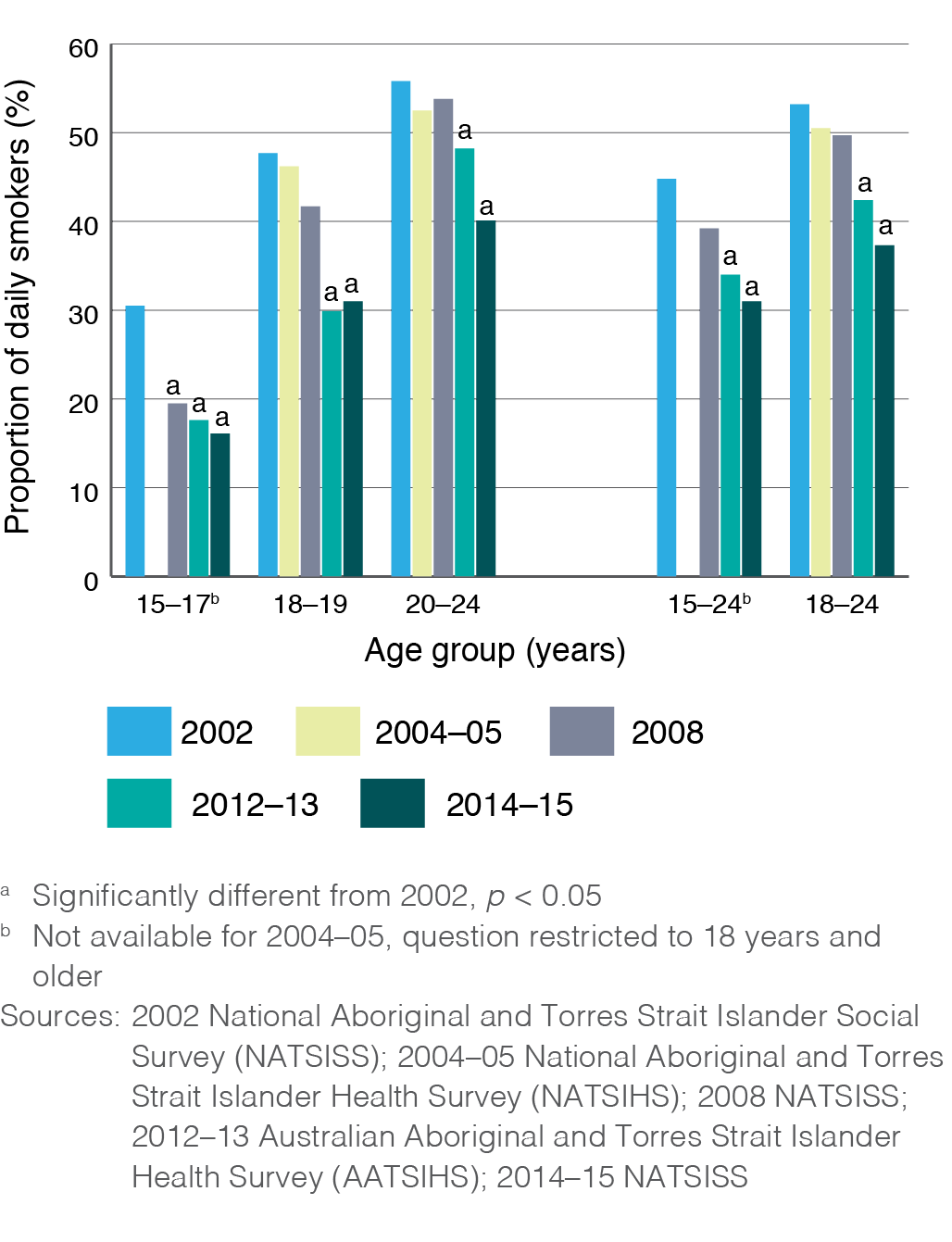
Between 2002 and 2014–15, daily smoking prevalence declined significantly among young people aged 15–24, from 45% down to 31%, a reduction of 14 percentage points (95% confidence interval [CI] 8, 21) (see Figure 1). Within this age range there were also significant decreases among 18–24-year-olds and all age subgroups (15–17, 18–19 and 20–24 years). The greatest magnitude of change was for 18–19-year-olds, a 17 percentage point decline between 2002 and 2014–15 (95% CI 4, 29), down from 48% to 31%.
Figure 1. Proportion of Indigenous adolescents and young adults aged 15–24 years who smoked daily, 2002 to 2014–15 (click to enlarge)
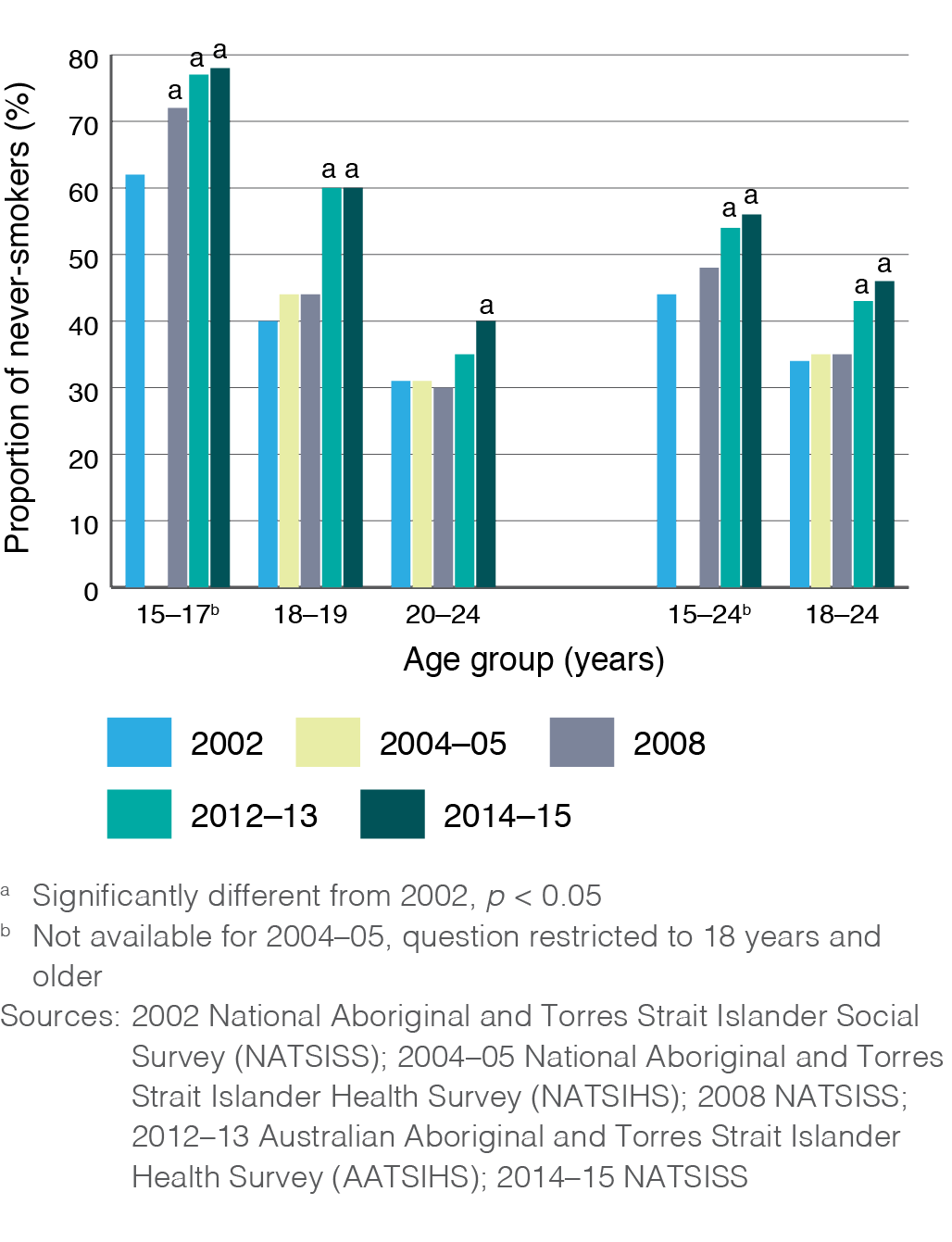
The proportion of never-smokers among 15–24-year-olds increased significantly, by 12 percentage points (95% CI 6, 18) from 44% in 2002 to 56% in 2014–15 (see Figure 2). As with daily smoking, there were significant changes for all age subgroups, and the greatest change was among 18–19-year-olds with a 20 percentage point increase (95% CI 7, 32) in never smoking from 40% in 2002 to 60% in 2014–15.
Figure 2. Proportion of Indigenous adolescents and young adults aged 15–24 years who have never smoked, 2002 to 2014–2015 (click to enlarge)
Changes in the age daily smoking started
For all respondents aged 18 years and older who have ever smoked daily, the age daily smoking commenced did not change between 2004–05 and 2012–13, with the majority (70%) starting before 18 years of age and around 30% starting before age 15.
To investigate trends among more recently established smokers, we concentrated on 18–24-year-olds. We found significant declines between surveys in the proportions commencing smoking before age 18. In 2004–05, 84% of young people aged 18–24 years had started smoking daily before age 18; in 2012–13, the proportion had fallen to 76%, an 8 percentage point difference (95% CI 2, 15) (see Table 1). There was a nonsignificant decline in the proportion starting before age 15, down 8 percentage points (95% CI 0, 15) from 34% in 2004–05 to 26% in 2012–13.
Within the 18–24 years age group, there was a significant decrease of 9 percentage points (95% CI 1, 17) in the proportion of 20–24-year-olds who started smoking before 18 years of age. There was a nonsignificant decrease (4 percentage points; 95% CI −5, 13) among 18–19-year-olds. Both Western Australia (WA) and Victoria had significant reductions in the proportion of 18–24-year-olds starting smoking before age 18: a decline of 28 percentage points in Victoria (from 91% in 2004–05 to 63% in 2012–13) and 17 percentage points in WA (from 89% to 72%). There were also nonsignificant declines in almost all other age categories.
Table 1. Proportion of current and ex-daily smokers who started daily smoking before age 18, Indigenous respondents aged 18–24 years (N = 660)
| Variable | 2004–05
% n |
2012–13
% n |
Difference 2004–05 to 2012–13 Percentage points (95% CI) |
||
| Age | |||||
| Total 18–24 years | 84 | 554 | 76 | 391 | –8 (–15, –2)ª |
| 18–19 years | 92 | 159 | 88 | 110 | –4 (–13, 5) |
| 20–24 years | 81 | 395 | 72 | 281 | –9 (–17, –1)ª |
| Gender | |||||
| Male | 84 | 227 | 75 | 163 | –10 (–20, 0) |
| Female | 84 | 327 | 77 | 228 | –7 (–15, 1) |
| Location | |||||
| Remote | 78 | 178 | 65 | 149 | –12 (–24, 0) |
| Non-remote | 86 | 376 | 79 | 242 | –7 (–15, 0) |
| State/territory | |||||
| NSW | 86 | 92 | 89 | 73 | 3 (–6, 13) |
| Vic | 91 | 72 | 63 | 23 | –28 (–48, –8)ª |
| Qld | 80 | 101 | 68 | 71 | –12 (–28, 4) |
| SA | 85 | 55 | 79 | 44 | –6 (–27, 15) |
| WA | 89 | 90 | 72 | 65 | –17 (–30, –5)ª |
| NT | 75 | 70 | 64 | 68 | –12 (–29, 5) |
a Statistically significant difference, p < 0.05
Sources: 2004–05 National Aboriginal and Torres Strait Islander Health Survey (NATSIHS), 2012–13 Australian Aboriginal and Torres Strait Islander Health Survey (AATSIHS)
Among current and ex-daily smokers who started smoking daily before age 18, there were no consistent differences between the groups in each of the 10-year age/birth cohorts, either between or within survey waves, with one exception: a higher proportion of 20–29-year-olds started smoking before age 18 compared with the 30–39-year-old group (see Supplementary Table 2, available from: doi.org/10.26188/5c99c69983651).
Discussion
Our results demonstrate that fewer young Indigenous people are taking up smoking, and, of those who do, an increasing proportion are starting daily smoking later, after age 18. This appears to be a recent change.
These findings add to recent reports of the decline in smoking among Indigenous people over the past 10–15 years3,5,21, particularly young people, largely due to the increase in the proportion of never-smokers. This will have substantial health benefits for Indigenous people because nonsmokers live 10 years longer on average than smokers.22 With increases in the number of lifelong never-smokers alongside thousands of people who have quit, the burden from premature mortality and tobacco-related illnesses will decline.5,21
Sustaining and accelerating this progress requires continued commitment to the comprehensive tobacco control approach that has supported these improvements for young people in particular.5,21 It is not possible to determine if any individual component has been more effective than others, but measures that are Indigenous-led and culturally tailored are identified as particularly important.21,23 A greater understanding of what works for young people of different ages is needed to design programs that continue to prevent smoking throughout adolescence and into adulthood.23
Our results may indicate a trend towards delayed smoking initiation, with the largest increase in never smoking since 2002 among 18–19-year-olds and more moderate changes among 20–24-year-olds. As shown previously for both Indigenous and non-Indigenous people5, we found that the majority of Indigenous adolescents and young adults who have ever smoked regularly started smoking before age 18. However, our analysis found an increasing number of people commencing after 18 years of age. This is similar to changes in the broader population, in which the average age for the first full cigarette smoked increased to 16 years in 2016, up from 14 years in 1995, and the proportion of people older than 18 years trying smoking for the first time increased significantly from 28% in 2013 to 31% in 2016 (increasing steadily from 18% in 2004).11 Our results suggest a more recent shift among Indigenous adolescents and young adults, with no significant differences between age cohorts except the greater proportion of 20–29-year-olds starting daily smoking before age 18 years, as expected for existing smokers in their 20s.
Based on the initiation model described earlier, our results suggest a potential shift from ‘early’ to ‘late establishers’, or possibly an increase in age for all categories. There may be some relative positive health impacts of fewer smokers commencing in early adolescence, as those who start earlier are less likely to make successful quit attempts24,25, are more likely to become heavy smokers and to develop tobacco-related diseases.7
Despite the relative benefits of delayed smoking initiation, preventing later uptake and progression to long-term smoking is nonetheless important. The risk and protective factors for smoking change throughout adolescence and young adulthood, and the transition is a period of increased vulnerability and susceptibility to smoking uptake.10 New risk factors for smoking may be introduced, and previously protective influences diminished as young people enter early adulthood: leaving school and home, and starting work, study, households and families. Previously positive influences of smoke-free homes and cars, family attitudes to smoking, engagement with school and sport, and exposure to youth-focused health promotion may be replaced by new smoking norms at home, work and among friends, along with greater access to cigarettes (due to age and income).
There may also be some time-specific factors. The changes reported here are for a group aged 18–24 years in 2012–13. That is, their smoking was established before, or during, the renewed national focus on tobacco control following a peak in tobacco control activities in the late 1990s to early 2000s. Funding for the Tackling Indigenous Smoking program began in 2010; the first Indigenous targeted social marketing campaign, Break the Chain, aired in 2011; mainstream campaign activity increased from 2012; tobacco plain packaging was introduced in 2012; and the annual excise on tobacco increased from 2013.
Is it possible that this cohort progressed through adolescence with lower exposure to health promotion and social marketing, particularly Indigenous-led tobacco control, and were more susceptible to smoking uptake as they entered young adulthood? Or perhaps the effect of measures that prevented uptake during their teenage years was not sustained, contributing to later smoking initiation and a renormalisation of smoking in this age group? Increased understanding of the factors that influence smoking uptake for young Indigenous people during the transition into adulthood, and what measures are effective to reduce uptake, is required, including the unique determinants of smoking initiation for this population within the historical context of colonisation.26 It is necessary to invest in, and where required adapt, health promotion programs and policies to ensure tobacco prevention and cessation supports are effective and culturally relevant for Indigenous adolescents. Further, it is important to ensure smoke-free messages are reinforced and remain relevant across all stages of adolescence and young adulthood, and continue to reduce smoking initiation, not just delay it.
Strengths and limitations
A strength of this work is that it reports data that are not routinely published, from a nationally representative sample of Indigenous people, including those in remote areas. However, there are some limitations. The surveys sample people living in private residences, which excludes hospitals, correctional facilities, hostels, other short-stay accommodation and boarding schools. For some subgroups, the sample sizes and changes are insufficient to detect potentially important differences. While some outcomes are analysed by remoteness or state/territory, the data are primarily reported at a national level, which does not allow identification of regional variation. There were minor changes in questions about smoking status and initiation between remote and nonremote areas and between surveys. The definition of ‘never smoking’ differed between the NATSISS and the NATSIHS/AATSIHS; however, the definition is consistent in our comparisons between 2002 and 2014–15.
The analysis of the age that daily smoking commenced includes only two time points. We used birth cohort comparisons to demonstrate that the detected differences in later uptake appear to be a recent change. While significant differences have been detected, they should be interpreted with caution; the analysis should be repeated when a third wave of this ABS data is available to provide greater certainty. In the interim, qualitative research may facilitate an in-depth exploration of the experiences leading to later smoking uptake and any relevant time-period factors.
Conclusions
Smoking prevalence among young Indigenous people has been declining since 2002, with a growing number of never-smokers. However, nonsmoking adolescents entering young adulthood may still be susceptible to starting smoking. Primary health care sevices cannot assume that a client who previously presented as a never-smoker in their late teens or early 20s will remain so. Nor can it be assumed that activities that have been effective in driving down youth smoking rates continue to be effective with young adults.
Influences on smoking initiation change throughout adolescence and young adulthood. While our results show that most daily smoking continues to be established before age 18, around one-quarter of smokers start before 15 years of age, a similar proportion start after 18 years (and that may be increasing), with the remaining 50% starting between 15 and 17 years.
Commitment to the comprehensive tobacco control measures that have contributed to the reduction in youth smoking must be sustained, and Indigenous-led prevention must be prioritised to ensure cultural relevance. Our results suggest that these interventions need to continue across all of adolescence and young adulthood, reinforcing tobacco prevention at very different life stages, to ensure smoking uptake continues to decline and is not simply delayed.
Acknowledgements
Funding was provided to VACCHO by the Victorian Department of Health and Human Services for a broader project including this research, and provided travel support for authors. A portion of this funding was provided to the Menzies School of Health Research for completion of the analysis. CH receives a PhD scholarship from The Australian Prevention Partnership Centre funded through the National Health and Medical Research Council Partnership Centre grant scheme (Grant ID: GNT9100001).
Peer review and provenance
Externally peer reviewed, not commissioned.
Copyright:

© 2019 Heris et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Australian Institute of Health and Welfare. Australian burden of disease study: impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2011. Canberra: AIHW; 2016 [cited 2018 Mar 5]. Available from: www.aihw.gov.au/reports/burden-of-disease/australian-bod-study-2011-indigenous-australians
- 2. van der Sterren A, Greenhalgh EM, Knoche D, Winstanley MH. Prevalence of tobacco use among Aboriginal and Torres Strait Islander people. In: Scollo MM, Winstanley MH, editors. Tobacco in Australia: facts and issues. Melbourne: Cancer Council Victoria; 2016 [cited 2018 Aug 3]. Available from: www.tobaccoinaustralia.org.au/chapter-8-aptsi/8-3-prevalence-of-tobacco-use-among-aboriginal-peo
- 3. Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander Social Survey, 2014–15. Canberra: ABS; 2016 [cited 2018 Mar 5]. Available from: www.abs.gov.au/ausstats/[email protected]/mf/4714.0
- 4. Australian Health Ministers' Advisory Council. Aboriginal and Torres Strait Islander Health Performance Framework 2017 report. Canberra: AHMAC; 2017 [cited 2018 Mar 5]. Available from: www.niaa.gov.au/sites/default/files/publications/2017-health-performance-framework-report_1.pdf
- 5. Australian Bureau of Statistics. Aboriginal and Torres Strait Islander peoples: smoking trends, Australia, 1994 to 2014–15. Canberra: ABS; 2017 [cited 2018 Mar 5]. Available from: www.abs.gov.au/ausstats/[email protected]/mf/4737.0
- 6. Sawyer SM, Afifi RA, Bearinger LH, Blakemore S-J, Dick B, Ezeh AC, et al. Adolescence: a foundation for future health. Lancet. 2012;379(9826):1630–40. CrossRef | PubMed
- 7. US Department of Health and Human Services. Preventing tobacco use among young people: a report of the surgeon general. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2012 [cited 2018 Apr 4]. Available from: www.surgeongeneral.gov/library/reports/preventing-youth-tobacco-use/full-report.pdf
- 8. Choi WS, Gilpin EA, Farkas AJ, Pierce JP. Determining the probability of future smoking among adolescents. Addiction. 2001;96(2):313–23. CrossRef | PubMed
- 9. Messer K, Pierce JP. Changes in age trajectories of smoking experimentation during the California Tobacco Control Program. Am J Public Health. 2010;100(7):1298–306. CrossRef | PubMed
- 10. Winstanley M, Wood L, Greenhalgh E, Letcher T. Influences on the uptake and prevention of smoking. In: Scollo MM, Winstanley MH, editors. Tobacco in Australia: facts and issues. Melbourne: Cancer Council Victoria; 2014 [cited 2018 Mar 5]. Available from: www.tobaccoinaustralia.org.au/chapter-5-uptake
- 11. Australian Institute of Health and Welfare. National drug strategy household survey 2016: detailed findings. Canberra: AIHW; 2017 [cited 2018 Mar 5]. Available from: www.aihw.gov.au/getmedia/15db8c15-7062-4cde-bfa4-3c2079f30af3/21028a.pdf.aspx?inline=true
- 12. Australian Institute of Health and Welfare. Tobacco indicators: measuring midpoint progress. Reporting under the national tobacco strategy 2012–2018. Canberra: AIHW; 2016 [cited 2018 Mar 5]. Available from: www.aihw.gov.au/getmedia/fcf4f834-8ef8-44a0-99cb-8fc28150428d/20065.pdf.aspx?inline=true
- 13. Australian Bureau of Statistics. The Australian statistical geography standard (ASGS) remoteness structure. Canberra: ABS; 2018 [updated 15 Mar 2018; cited 2018 Mar 23]. Available from: www.abs.gov.au/websitedbs/d3310114.nsf/home/remoteness+structure
- 14. Australian Bureau of Statistics. Estimates of Aboriginal and Torres Strait Islander Australians, June 2011. Canberra: ABS; 2013 [cited 2018 Mar 5]. Available from: www.abs.gov.au/AUSSTATS/[email protected]/Lookup/3238.0.55.001Main+Features1June%202011?OpenDocument
- 15. Australian Bureau of Statistics. Australian Aboriginal and Torres Strait Islander health survey: users' guide, 2012–13. Canberra: ABS; 2013 [cited 2018 Mar 5]. Available from: www.abs.gov.au/AUSSTATS/[email protected]/Lookup/4727.0.55.002Main+Features12012-13
- 16. Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander health survey: users' guide, 2004–05. Canberra: ABS; 2006 [cited 2018 Mar 5]. Available from: www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/8B24B5C90B33D2BFCA257164007FCC1D/$File/4715055004_2004-05.pdf
- 17. Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander social survey, 2002. Canberra: ABS; 2004 [cited 2018 Mar 5]. Available from: www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/AE3942DB21AD4A27CA256EBB0079843D/$File/47140_2002.pdf
- 18. Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander social survey: users' guide, 2008. Canberra: ABS; 2010 [cited 2018 Mar 5]. Available from: www.abs.gov.au/AUSSTATS/[email protected]/Lookup/4720.0Main+Features12008
- 19. Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander social survey: user guide, 2014–15. Canberra: ABS; 2016 [cited 2018 Mar 5]. Available from: www.abs.gov.au/ausstats/[email protected]/PrimaryMainFeatures/4720.0
- 20. Donath SM. How to calculate standard errors for population estimates based on Australian National Health Survey data. Aust N Z J Public Health. 2005;29(6):565–71. CrossRef | PubMed
- 21. Lovett R, Thurber K, Wright A, Maddox R, Banks E. Deadly progress: changes in Australian Aboriginal and Torres Strait Islander adult daily smoking, 2004–2015. Public Health Res Pract. 2017;27(5):e2751742. CrossRef
- 22. Banks E, Joshy G, Weber MF, Liu B, Grenfell R, Egger S, et al. Tobacco smoking and all-cause mortality in a large Australian cohort study: findings from a mature epidemic with current low smoking prevalence. BMC Medicine. 2015;13(1):38. CrossRef | PubMed
- 23. Chamberlain C, Perlen S, Brennan S, Rychetnik L, Thomas D, Maddox R, et al. Evidence for a comprehensive approach to Aboriginal tobacco control to maintain the decline in smoking: an overview of reviews among Indigenous peoples. Systematic Reviews. 2017;6(1):135. CrossRef | PubMed
- 24. Breslau N, Peterson EL. Smoking cessation in young adults: age at initiation of cigarette smoking and other suspected influences. Am J Public Health. 1996;86(2):214–20. CrossRef | PubMed
- 25. Greenhalgh EM, Stillman S, Ford C. Factors that predict success or failure in quit attempts. In: Scollo MM, Winstanley MH, editors. Tobacco in Australia: facts and issues. Melbourne: Cancer Council Victoria; 2016 [cited 2018 Mar 5]. Available from: www.tobaccoinaustralia.org.au/chapter-7-cessation/7-7-personal-factors-associated-with-quitting
- 26. Lovett R, Thurber KA, Maddox R. The Aboriginal and Torres Strait Islander smoking epidemic: what stage are we at, and what does it mean? Public Health Res Pract. 2017;27(4):e2741733. CrossRef | PubMed