Abstract
Objectives: The jurisdictional nature of routinely collected health data in Australia has created challenges for linking data across state/territory and federal government boundaries. This has impeded understanding of the interplay between service use across hospital and community care. Our objective was to demonstrate the value-add of cross-jurisdictional data using a case study of health service use and the factors associated with healthcare use towards the end of life.
Study type: Retrospective cohort study using routinely collected health data.
Methods: We used two decedent cohorts of people aged ≥65 years who died in New South Wales (NSW), Australia, in 2006 or 2007. The population cohort comprised the general NSW population linked to NSW data collections; the other cohort comprised Australian Government Department of Veterans’ Affairs (DVA) clients (with full healthcare entitlements) linked to NSW and Commonwealth data. We compared information available on health services received during the last 6 months of life and ran multivariable analyses for both cohorts to demonstrate the added value of the Commonwealth data.
Results: We included 37 567 decedents in the population cohort and 11 259 in the DVA cohort. Cancer was the cause of death for 27% of the NSW cohort and 22% of the DVA cohort; approximately 40% of decedents in each cohort had a cancer history. We summarise information on hospital services for both cohorts and examine community care (general practitioner consultations, specialist presentations, prescriptions dispensed) for the DVA cohort only. Multivariable analyses in the DVA cohort demonstrated that high rates of emergency department (ED) presentations and hospitalisation were associated with higher rates of use of all health services, including community care. Use of primary care did not reduce ED or hospital use. We were not able to examine the interplay between community and hospital care in the NSW population cohort.
Conclusions: In our case study, we demonstrated the value-add of Commonwealth data for understanding the drivers of hospital services use, which has implications for service delivery and resource allocation. There is an abundance of routinely collected health data in Australia that can be used to describe whole-of-healthcare use for a broad range of issues.
Full text
Introduction
Routinely collected health data are a powerful tool for describing healthcare delivery for different population groups.1,2 Despite Australia’s universal healthcare system, whole-of-healthcare research is notoriously challenging because of the fragmented nature of data collections. Specifically, hospital datasets, including admissions and emergency department (ED) visits, are under the custodianship of individual states and territories, but health services delivered in the community and medicines – through the Medicare Benefits Scheme (MBS) and the Pharmaceutical Benefits Scheme (PBS) – are under the custodianship of the federal government (henceforth referred to as the Commonwealth).
Linking Australian data across jurisdictional boundaries has been made possible in recent years by the establishment of Commonwealth–approved integrating authorities. However, accessing cross-jurisdictional data for the entire population remains time-consuming and costly, meaning that researchers are faced with a trade-off between accessing cross-jurisdictional data for subsets of the population or accessing data for the whole population from the perspective of a sole healthcare payer – for example, the New South Wales (NSW) Government. For example, research on end-of-life care (the most resource-intensive period of care across the lifespan) in Australia has primarily focused on hospital services and place of death.3-9 Our previous work on end-of-life care for all adult decedents in Australia’s most populous state (NSW) highlighted several gaps where additional information (such as MBS and PBS data) is required to understand the interplay between hospital and community care.10,11 The exception to this is a program of research on end-of-life care for elderly cancer decedents using data from the Australian Government Department of Veterans’ Affairs (DVA).12,13As the sole payer of health services for its clients, the DVA maintains custodianship of a variety of routine data collections, so that research using DVA data provides a whole-of-health system description of end-of-life care. However, it is limited to a subset of the population, representing a small percentage of Australians older than 65 years of age.14,15
The aim of this study was to demonstrate the potential of linking cross-jurisdictional Australian routinely collected health administrative data using the case study of health service use at the end of life. We used data for two cohorts of decedents: for the DVA cohort, information on nearly all health services was available, whereas, for the NSW population cohort, only information on hospital-based care was available. We sought to quantify the gaps in state-level datasets and describe the benefit of additional information from Commonwealth data when seeking to understand the nature and extent of health service use. We used multivariable regression analysis to examine whether additional data could clarify the links between hospital and community care, and thus provide more comprehensive information to support service planning and delivery in Australia.
Methods
Setting
The Australian healthcare system entitles all citizens and permanent residents to a range of subsidised health services. This includes outpatient services such as consultations with medical and selected healthcare professionals (through the MBS), and medicines prescribed in hospitals and the community (through the PBS and hospital budgets). DVA funds the healthcare of eligible veterans, war widows and widowers, and their dependants. DVA clients have access to the universal healthcare arrangements provided to all Australian permanent residents and citizens, plus additional DVA-approved services and pharmaceutical items not subsidised for the general population.
Study samples
We used two previously described cohorts10-13, both based on health administrative data. To ensure that data were comparable across the two cohorts, our analysis was limited to people aged 65 years or older who died in NSW in 2007 (the ‘population cohort’) or in 2006–2007 (the ‘DVA cohort’); 2007 is the most recent year for which information on cause of death was available to our research group. The DVA cohort consisted only of clients with full healthcare entitlements, to allow capture of nearly all health services received.
Data sources and ethics
Data were linked by a third party using probabilistic, privacy-preserving protocols (Centre for Health Record Linkage [CHeReL], www.cherel.org.au). A comparison of the datasets available for both cohorts is summarised in Table 1. Additional information about these linked datasets for the population cohort10,11and DVA cohort12,13 has been published previously.
The NSW Population and Health Services Research Ethics Committee (approval number 2013/11/494) and the Department of Veterans’ Affairs Human Research Ethics Committee (approval number E013/015) approved the research using the DVA cohort. The NSW Population and Health Services Research Ethics Committee approved the research using the NSW population cohort (approval number LNR 2012/01/014).
Table 1. Datasets available for the population cohort and DVA cohort
X indicates that information was available
| Information | Dataset (jurisdiction) | Cohort | |
| Population | DVA | ||
| Cause of death | RBDM (NSW) | X | X |
| Cancer diagnoses received between 1994 and 2007 |
NSWCR (NSW) | X | X |
| Inpatient hospitalisationsa includes time spent in intensive care |
APDC (NSW) | X | X |
| Emergency department visitsb | EDDC (NSW) | X | X |
| Clinician visits and procedures | DVA health services file (Commonwealth) | X | |
| Prescription medicines dispensed | RPBS (Commonwealth) | X | |
| Residence in aged care facility | DVA residential aged care database (Commonwealth) | X |
APDC = Admitted Patient Data Collection; DVA = Department of Veterans’ Affairs; EDDC = Emergency Department Data Collection; NSWCR = New South Wales Cancer Registry; RBDM = Registry of Births, Deaths and Marriages (linked to coded cause of death information in the Australian Bureau of Statistics mortality data); RPBS = Repatriation Pharmaceutical Benefits Scheme
a The APDC covers inpatient separations from all public and private hospitals in NSW.
b Emergency department (ED) data did not cover all of NSW during the study period but did capture all of the larger EDs, accounting for around 80% of ED presentations. EDs in areas not covered are relatively small facilities. Only public hospitals contribute to the EDDC.
Measures and statistical analyses
DVA clients are included in the NSW population cohort, so we did not conduct formal statistical comparisons of cohort characteristics. We classified place of residence (Accessibility/Remoteness Index for Australia; ARIA+) and socio-economic status (Socio-Economic Indexes for Areas; SEIFA) based on the Statistical Local Area of residence at the time of death. Comparable data on morbidity are not presented because the Charlson index (based on hospitalisations)16 could not be calculated; information from eligible hospitalisations was not available for 62% of the NSW population cohort and 60% of the DVA cohort. We calculated the RxRisk morbidity17 index for the DVA cohort; this index calculates a morbidity score based on prescription medicines use.
Outcomes were reported during the last 6 months of life, based on 6 constructed ‘months’ consisting of 30 days each; the last ‘month’ included the date of death in the 30-day period.
We compared hospital-specific measures for the two study cohorts, including number of hospital admissions and ED presentations, time spent in hospital, admission to an intensive care unit (ICU) and admissions related to palliative care during both the last 6 months and the last 30 days of life.9 To demonstrate the usefulness of cross-jurisdictional linked data, we present a selection of additional information on health services received during the last 6 months of life for the DVA cohort, including physician visits and procedures, prescription medications such as opioids, and chemotherapy use (for cancer decedents).
Multivariable logistic regression models were fitted to determine factors associated with higher hospital use based on the distribution of hospital use in the population samples. The cut-point for the top quartile of use was three or more hospital admissions, or three or more ED visits during the last 6 months of life; this methodology was similar to our previous research examining care in the last 12 months of life.10 Three separate models were run for each of the outcomes: 1) the whole NSW cohort and associated data holdings; 2) the DVA cohort but limited to data available for the NSW cohort; and 3) the DVA cohort with data available from all sources. Comparisons of the results of these models allowed us to examine the generalisability of results in the DVA cohort to the NSW population aged 65 and older, and the value added by having access to cross-jurisdictional data to understand the association between use of selected community services and higher hospital use. Factors included in all three models were age at death, sex, place of residence, socio-economic status, cancer history and cause of death. The third model also included community-based health services that have been shown to be associated with reduced hospital use18 (general practitioner [GP] and specialist consultations).
A condensed version of the results is provided in this manuscript. For comprehensive data tables, please see the online supplement (available from https://handle.unsw.edu.au/1959.4/unsworks_48988).
Analyses were carried out in SAS (Cary, North Carolina: SAS Institute Inc; version 9.3).
Results
Cohort characteristics
A total of 37 567 decedents met the inclusion criteria for the population cohort and 11 259 for the DVA cohort. Decedents in the DVA cohort were generally older (median age 86 vs 83 years) and more commonly male (60% vs 48%) than the population cohort. For both cohorts, about 40% of decedents had a previous cancer diagnosis, with cancer accounting for 27% of deaths in the population cohort and 22% in the DVA cohort. Hospital or an identified inpatient hospice was the most common place of death (approximately 50% for both cohorts) (see Supplementary Table 1, available from: https://handle.unsw.edu.au/1959.4/unsworks_48988).
The value-add of cross-jurisdictional data for understanding health services use in the last 6 months of life
During the last 6 months of life, the number and duration of hospital admissions were similar for both cohorts, but the DVA cohort had a slightly lower proportion of decedents who were admitted to the ICU or had at least one palliative care–related admission.
During the last 30 days of life, both cohorts had similar hospital use; however, twice the percentage of decedents in the DVA cohort had two or more hospital episodes of care.
For decedents in the DVA cohort, we summarised some examples of the additional information on out-of-hospital health services used during the last 6 months of life, including prescription medicines, community-based services and GP visits by location (see Supplementary Tables 2 and 3, available from: https://handle.unsw.edu.au/1959.4/unsworks_48988).
The value-add of cross-jurisdictional data for understanding factors associated with increased hospital admissions in the last 6 months of life
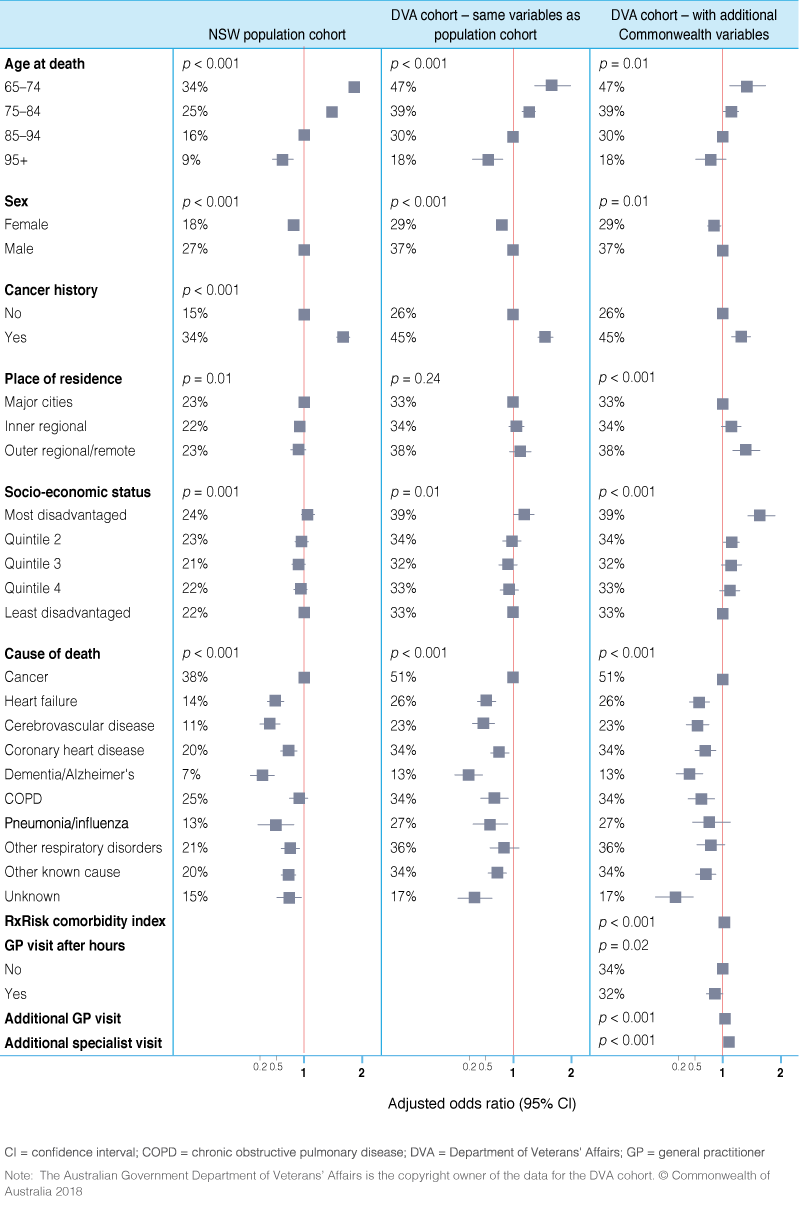
The results of multivariable analyses suggest that, for the NSW population cohort, younger age at death and having a cancer history were associated with a greater likelihood of having three or more hospital admissions (Figure 1). Decedents who were female, lived outside major cities, or died from conditions other than cancer were significantly less likely to be admitted to hospital three or more times. Similar factors were associated with higher hospital use for the DVA cohort, when the analysis was restricted to NSW data holdings. When the analysis for the DVA cohort was expanded to include additional Commonwealth data holdings, we found that having at least one after-hours GP visit meant that decedents were less likely to have more hospital admissions. However, overall, larger numbers of GP and specialist visits were associated with an increased likelihood of higher numbers of hospital admissions.
Figure 1. Associations between cohort characteristics and ≥3 hospital episodes during the last 6 months of life for the population cohort and DVA cohort (click to enlarge)
The value-add of cross-jurisdictional data for understanding factors associated with increased ED presentations in the last 6 months of life
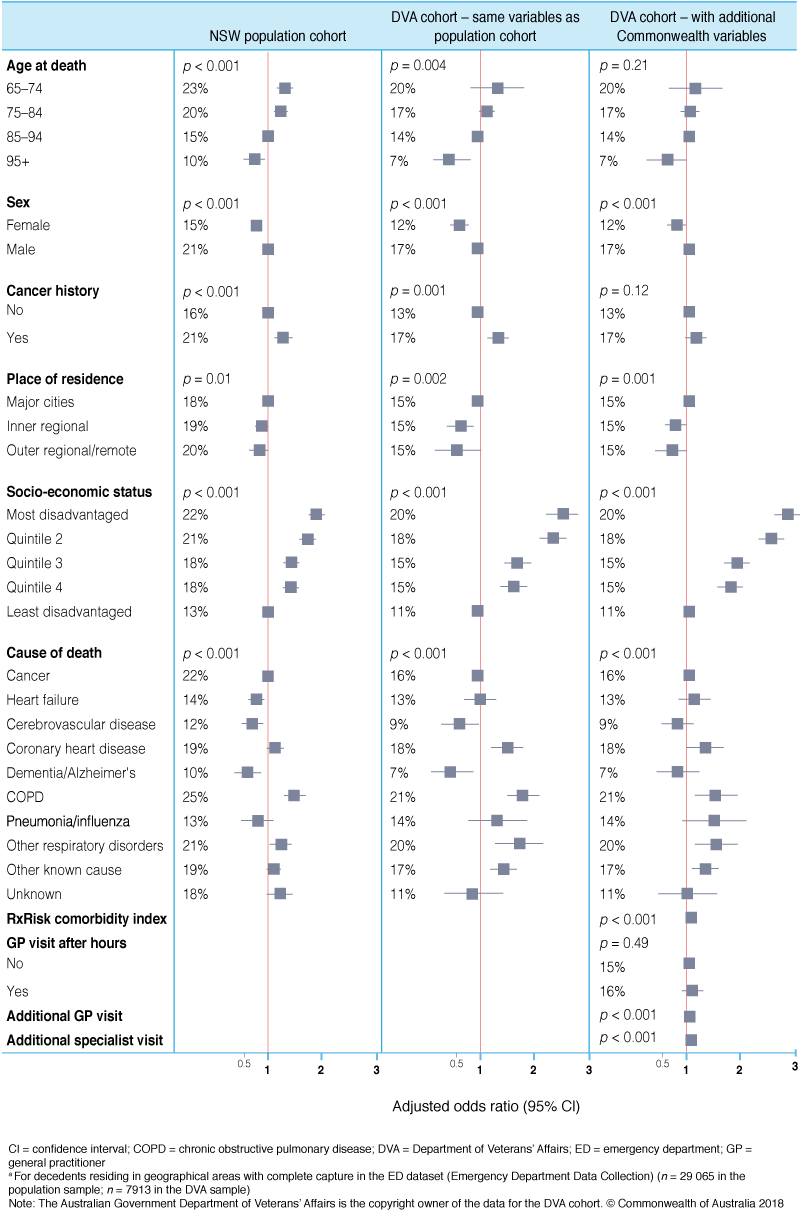
The following factors were significantly associated with higher ED use in both cohorts (analyses restricted to NSW datasets): being younger at death, having a cancer history, being male, and dying from chronic obstructive pulmonary disease or other respiratory disorders (Figure 2). There was a clear relationship between socio-economic status and higher ED use, with those living in the most disadvantaged areas having nearly twice the odds of being high users of the ED compared with those living in the least disadvantaged areas. When the analysis of the DVA cohort was expanded to include additional Commonwealth data holdings, we found no association between after-hours GP visits and higher ED use. However, larger numbers of GP and specialist visits were associated with an increased likelihood of higher ED use.
Figure 2. Associations between cohort characteristics and ≥3 ED presentationsa during the last 6 months of life for the population cohort and DVA cohort (click to enlarge)
Discussion
In this study, we focused on end-of-life care to demonstrate the added value of comprehensive, linked cross-jurisdictional data to examine resource use in the last 6 months of life, particularly the drivers of high use of hospital services.
For the population cohort (with NSW data holdings only), we were limited to data about hospital-based services, whereas for the DVA cohort we were able to examine a more comprehensive range of health services, including hospitalisations, community-based care and prescription medicine use. Importantly, the linkage of community and hospital data allowed us to further examine the association between increased use of hospital services and use of community care.
The additional data available for the DVA cohort allowed us to explore important questions about end-of-life care, which have the potential to inform service delivery and resource allocation decisions. In Australia, as in similar jurisdictions internationally, there is increasing pressure to reduce the burden on hospital systems and, where possible, effectively manage patients in the community. This is particularly important because hospitalisations account for the vast majority of end-of-life costs.13 In this paper, we identified particular patient groups (e.g. cancer patients, those living in disadvantaged areas of NSW) who are more likely to use hospital services extensively at the end of life. By examining the association between selected community-based services (GP and specialist visits) and high hospital and ED use, we found that after-hours GP visits were associated with a lower likelihood of high hospital use. However, in general, high use of hospital services was associated with high use of community care during the last 6 months of life. This finding was contrary to our expectation that use of community-based services may be associated with reduced hospitalisations; it might suggest that patients using hospital services repeatedly at the end of life may be using more services overall. However, we could not examine continuity of physician care or the number of providers, which may modify the associations we observed.18-20
Despite the comprehensive data holdings for the DVA cohort (or any cohort with linkages across Commonwealth and state/territory boundaries) there remain some data gaps, such as community-based palliative care. The fragmented nature of palliative care data holdings across hospital and community settings, and the lack of clinical information in MBS data (physician visits, community nursing) are limitations of our current data holdings.10,13 Such data are vital to fully understanding the nature and extent of end-of-life care.
The presentation of results from two programs of work with different data holdings allowed, for the first time, comparison of end-of-life health service use by DVA clients and the general population. Previous research examining health service use more generally has found that DVA clients have similar rates of health service use when compared with Australians of a similar age14,15; this study suggests that the same is true for end-of-life hospital care.
Although the results were similar for the two population samples, the characteristics of the DVA population (average age of 75 years in 2014) means that there are missed opportunities to understand whole-of-healthcare use in the broader Australian population. This is also true of other research disciplines using routinely collected data in Australia, including pharmacoepidemiology, for which we recently demonstrated that almost all the studies examining outcomes associated with medicines prescribed in the community (requiring linkage of PBS data to hospital and death data from the states) were limited to DVA clients.21 We suggest that it would be beneficial if datasets comprising hospitalisations, community care and prescription medicines were linked across the entire Australian population to add to the comprehensive research that has been undertaken using DVA data holdings. There is great value in accessing these data, but the limitations of using administrative data, usually collected for purposes other than research, are well recognised (e.g. time lag in access to data, quality of clinical information). However, as researchers have more access to, and experience using, these data, methods (including validated indicators and risk adjustment methods) continue to improve.
Conclusion
In Australia, there are currently barriers to accessing and using comprehensive linked health data crossing community and hospital care. Similar challenges are faced internationally. For example, a recent comparison of end-of-life care in seven developed countries using health administrative data was limited to hospital-based care, and only two of the seven countries were able to report data after 2010.22 Fragmented data collections, lack of national minimum datasets to enable national comparisons, and the concerns of stakeholders (patients and providers) have been cited as barriers to data access in regions such as the UK, Canada and the US.1,2,23,24 Australia, like most developed countries, has data protection and information governance legislation, but these were not determined with big data in mind. As the landscape and potential of big data evolve, engagement of key stakeholders to achieve the right balance between the benefits and risks of the use of this type of data is an important future priority.2
Acknowledgements
We thank DVA, the Cancer Institute NSW, the NSW Ministry of Health and the Centre for Health Record Linkage for access to, and linkage of, the datasets for this study. This research is supported by a National Health and Medical Research Council (NHMRC) Capacity Building Grant (ID: 571926), the NHMRC Centre of Research Excellence in Medicines and Ageing (ID: 1060407), a Cancer Australia Priority Driven Collaborative Research Grant (ID: 1050648), and the Cancer Institute NSW via a NSW Oncology Group Project Support Application. SAP is supported by a Cancer Institute NSW Career Development Fellowship (ID 12/CDF/2-25), and JI conducted this research with funding support from the Cancer Institute NSW Academic Chairs Program.
Disclaimer
The Australian Government Department of Veterans’ Affairs is the copyright owner of the data for the DVA cohort contained in this manuscript including all tables, figures and supplementary content. The authors have obtained permission from the Australian Government Department of Veterans’ Affairs to publish this manuscript. The views expressed in this version of the work do not necessarily represent the views of the Minister for Veterans’ Affairs or the Department of Veterans’ Affairs. The Commonwealth of Australia does not give any warranty nor accept any liability in relation to the contents of this work. The views expressed in this work do not necessarily represent the views of the Cancer Institute New South Wales.
Copyright:

© 2018 Commonwealth of Australia (with respect to the data for the Australian Government Department of Veterans’ Affairs cohort contained in the manuscript) and Langton et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Bates DW, Saria S, Ohno-Machado L, Shah A, Escobar G. Big data in health care: using analytics to identify and manage high-risk and high-cost patients. Health Aff (Millwood). 2014;33(7):1123–31. CrossRef | PubMed
- 2. Heitmueller A, Henderson S, Warburton W, Elmagarmid A, Pentland AS, Darzi A. Developing public policy to advance the use of big data in health care. Health Aff (Millwood). 2014;33(9):1523–30. CrossRef | PubMed
- 3. Kardamanidis K, Lim K, Da Cunha C, Taylor LK, Jorm LR. Hospital costs of older people in New South Wales in the last year of life. Med J Aust. 2007;187(7):383–6. PubMed
- 4. Rosenwax LK, McNamara BA, Murray K, McCabe RJ, Aoun SM, Currow DC. Hospital and emergency department use in the last year of life: a baseline for future modifications to end-of-life care. Med J Aust. 2011;194(11):570–3. PubMed
- 5. Calver J, Bulsara M, Boldy D. In-patient hospital use in the last years of life: a Western Australian population-based study. Aust N Z J Public Health. 2006;30(2):143–6. CrossRef | PubMed
- 6. Currow DC, Burns CM, Abernethy AP. Place of death for people with noncancer and cancer illness in South Australia: a population-based survey. J Palliat Care. 2008;24(3):144–50. PubMed
- 7. McNamara B, Rosenwax L. Factors affecting place of death in Western Australia. Health Place. 2007;13(2):356–67. CrossRef | PubMed
- 8. Moorin RE, Holman CDJ. The cost of in-patient care in Western Australia in the last years of life: a population-based data linkage study. Health Policy. 2008;85(3):380–90. CrossRef | PubMed
- 9. Langton JM, Blanch B, Drew AK, Haas M, Ingham JM, Pearson SA. Retrospective studies of end-of-life resource utilization and costs in cancer care using health administrative data: a systematic review. Palliat Med. 2014;28(10):1167–96. CrossRef | PubMed
- 10. Goldsbury DE, O’Connell DL, Girgis A, Wilkinson A, Phillips JL, Davidson PM, Ingham JM. Acute hospital-based services used by adults during the last year of life in New South Wales, Australia: a population-based retrospective cohort study. BMC Health Serv Res. 2015;15(1):537. CrossRef | PubMed
- 11. O’Connell DL, Goldsbury DE, Davidson P, Girgis A, Phillips JL, Piza M, et al. Acute hospital-based services utilisation during the last year of life in New South Wales, Australia: methods for a population-based study. BMJ Open. 2014;4(3):e004455. CrossRef | PubMed
- 12. Langton JM, Srasuebkul P, Reeve R, Parkinson B, Gu Y, Buckley NA, et al. Resource use, costs and quality of end of life care: observations in a cohort of elderly Australian cancer decedents. Implement Sci. 2015;10(1):25. CrossRef | PubMed
- 13. Langton JM, Reeve R, Srasuebkul P, Haas M, Viney R, Currow D, Pearson SA. Health service use and costs in the last 6 months of life in elderly decedents with a history of cancer: a comprehensive analysis from a health payer perspective. Br J Cancer. 2016;114(11):1293–302. CrossRef | PubMed
- 14. Tooth LR, Hockey R, Treloar S, McClintock C, Dobson A. Does government subsidy for costs of medical and pharmaceutical services result in higher service utilization by older widowed women in Australia? BMC Health Serv Res. 2012;12(1):179. CrossRef | PubMed
- 15. Australian Institute of Health and Welfare. Health care usage and costs: a comparison of veterans and war widows and widowers with the rest of the community. Canberra, AIHW; 2002 [cited 2018 February 7]. Available from: www.aihw.gov.au/reports/health-welfare-expenditure/health-care-usage-and-costs-a-comparison-of-veter/formats
- 16. Sundararajan V, Henderson T, Perry C, Muggivan A, Quan H, Ghali WA. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004;57(12):1288–94. CrossRef | PubMed
- 17. Sloan KL, Sales AE, Liu C-F, Fishman P, Nichol P, Suzuki NT, Sharp ND. Construction and characteristics of the RxRisk-V: a VA-adapted pharmacy-based case-mix instrument. Med Care. 2003;41(6):761–74. CrossRef | PubMed
- 18. Burge F, Lawson B, Johnston G. Family physician continuity of care and emergency department use in end-of-life cancer care. Med Care. 2003;41(8):992–1001. CrossRef | PubMed
- 19. van Walraven C, Oake N, Jennings A, Forster AJ. The association between continuity of care and outcomes: a systematic and critical review. J Eval Clin Pract. 2010;16(5):947–56. CrossRef | PubMed
- 20. Almaawiy U, Pond GR, Sussman J, Brazil K, Seow H. Are family physician visits and continuity of care associated with acute care use at end-of-life? A population-based cohort study of homecare cancer patients. Palliat Med. 2014;28(2):176–83. CrossRef | PubMed
- 21. Pearson SA, Pesa N, Langton JM, Drew A, Faedo M, Robertson J. Studies using Australia’s Pharmaceutical Benefits Scheme data for pharmacoepidemiological research: a systematic review of the published literature (1987–2013). Pharmacoepidemiol Drug Saf. 2015;24(5):447–55. CrossRef | PubMed
- 22. Bekelman JE, Halpern SD, Blankart CR, Bynum JP, Cohen J, Fowler R, et al. Comparison of site of death, health care utilization, and hospital expenditures for patients dying with cancer in 7 developed countries. JAMA. 2016;315(3):272–83. CrossRef | PubMed
- 23. Sibbald SL, Singer PA, Upshur R, Martin DK. Priority setting: what constitutes success? A conceptual framework for successful priority setting. BMC Health Serv Res. 2009;9(1):43. CrossRef | PubMed
- 24. Hagger-Johnson GE, Harron K, Goldstein H, Parslow R, Dattani N, Borja MC, et al. Making a hash of data: what risks to privacy does the NHS’s care.data scheme pose? BMJ. 2014;348:g2264. CrossRef | PubMed