Abstract
Objective: To explore variation in public hospital rates of early (37−38 weeks gestation) prelabour repeat caesarean section among low-risk women at and beyond term in New South Wales (NSW) between 2008 and 2011.
Importance of the study: A NSW Ministry of Health policy directive for public hospitals (PD2007_024), ‘Maternity − timing of elective or pre-labour caesarean section’, requires that low-risk elective or prelabour caesarean section does not occur before 39 completed weeks gestation. However, compliance with this policy has not been evaluated.
Study type: Population-based record linkage study
Methods: Linked birth and hospital data for low-risk, prelabour repeat caesarean sections in NSW in 2008−2011 were analysed using multilevel regression modelling. Rates were adjusted for casemix and hospital factors. Low-risk pregnancies were defined as singleton live births at 37−42 weeks gestation among women without medical or obstetric complications and where the indication for caesarean section was ‘elective repeat caesarean section’.
Results: In 2008−2011, there were 15 163 prelabour repeat caesarean sections among low-risk women in NSW. Overall, 34.7% of low-risk prelabour repeat caesarean sections occurred before 39 weeks gestation. Adjusted NSW public hospital rates of early (37−38 weeks gestation) low-risk prelabour repeat caesarean section varied widely (16.3−67.5%). Adjusting for casemix factors actually increased the between-hospital variation by 4.3%; adjusting for hospital factors reduced variation by 20.0%. Smoking, private healthcare, assisted reproductive technology use, higher parity, a noncaesarean uterine scar and delivering in a hospital with CPAP (continuous positive airway pressure) facilities were associated with higher odds of early delivery, although infants that were small for gestational age were associated with lower odds. Hospitals with higher rates of low-risk deliveries and higher propensity for vaginal birth after caesarean section had lower odds of early delivery.
Conclusions: The findings suggest generally poor compliance with the policy directive that prelabour caesarean does not occur before 39 weeks gestation, with adjusted compliance rates ranging from 32.5% to 83.7%. Large between-hospital variation after adjustment suggests that nonmedical factors are related to timing of low-risk prelabour repeat caesarean sections. Further strategies are needed to improve adherence to this evidence based policy.
Full text
Introduction
Many international obstetric guidelines1-3, including those of the Royal Australian and New Zealand College of Obstetricians and Gynaecologists 2, recommend that low-risk prelabour caesarean sections be performed after 39 weeks gestation, because of the increased risk of respiratory and other adverse infant outcomes when babies are electively delivered before 39 weeks.4 In April 2007, the New South Wales (NSW) Ministry of Health released a mandatory policy directive for all NSW public hospitals (PD2007_024), ‘Maternity − timing of elective or pre-labour caesarean section’, requiring that “where there are no compelling medical indications, elective or prelabour caesarean section does not occur prior to 39 completed weeks gestation”.5
Although a slight change in timing of prelabour caesarean sections has been observed since 20086, current practice and compliance with the policy directive are unknown. Additionally, the relationship between hospital and patient factors and timing of low-risk caesarean sections has not been explored. This study aimed to explore variation in public hospital rates of early (37−38 weeks) prelabour repeat caesarean section among low-risk women at and beyond term in NSW between 2008 and 2011.
Methods
This study examined routinely collected NSW health data from 2008 to 2011, following the introduction of the policy (April 2007). Data were obtained from two linked Ministry of Health datasets: the NSW Perinatal Data Collection and the Admitted Patient Data Collection. Record linkage was undertaken by the NSW Centre for Health Record Linkage.7,8 The study population included all low-risk, prelabour caesarean births among women who had had a previous caesarean section (i.e. the indication for caesarean section was elective repeat). The study was limited to repeat caesarean sections to reduce the heterogeneity of populations within and between hospitals. Low-risk pregnancies were defined as singleton live births at term (37−42 weeks) among women without diabetes, hypertension, other chronic diseases or placental conditions, with no previous perinatal death or classical caesarean, and where the indication for caesarean section was ‘elective repeat caesarean section’. Private hospitals (NSW Health policy directives apply to public hospitals) and hospitals with fewer than 50 births per year were excluded. Gestational age (expressed as completed weeks of gestation) was based on the best clinical estimate using ultrasound examination and/or last menstruation period.
Casemix and hospital factors are potentially associated with the timing of elective repeat caesarean sections at term.9 The casemix variables available for analysis included maternal age, country of birth, smoking, socio-economic status, body mass index, private healthcare, number of previous caesarean sections, number of previous vaginal births, assisted reproductive technology use, previous noncaesarean uterine scar10 and infant size for gestational age. Hospital factors included obstetric training provision (primary − referring to tertiary obstetric training hospitals, or secondary − referring to large district and rural hospitals that host obstetric registrars), level of perinatal care (neonatal intensive care unit, continuous positive airway pressure [CPAP] facilities and CPAP-trained staff, other), location and birth volume. Hospital rates of obstetric transfusions, anaesthetic services and low-risk births were also used, as was the rate of vaginal birth after primary caesarean section for breech presentation as an indicator of hospital propensity for vaginal birth after caesarean.9,11 Variables from the birth record are considered to be reliably reported, and the coding of hospital diagnoses and procedures has previously been validated.12,14
Using methods detailed elsewhere11, we conducted multilevel regression modelling with the outcome ‘timing of low-risk prelabour repeat caesarean section’ (37−38 weeks was classified as ‘early delivery’, and 39−42 weeks was classified as ‘later delivery’). Briefly, multivariable, multilevel binomial logistic regression models were constructed with a manual backward stepwise approach. An unadjusted model included a random intercept for hospital, to account for clustering of observations from the same hospital, and a shrinkage factor to allow for inclusion of hospitals with small sample sizes. Models were fitted and progressively adjusted, first for casemix and then for hospital factors, as described previously.9,11 The final risk-adjusted hospital rates with 95% confidence intervals (CI) were plotted. The relative contributions of casemix and hospital factors to the overall reduction in variation were quantified by calculating the difference between the hospital variation of the current and preceding step as a proportion of the unadjusted model’s hospital variation.9,11 Adjusted odds ratios (aOR) and 95% CI for factors retained in the final model are reported. The study was approved by the NSW Population and Health Services Research Ethics Committee.
Results
Between 2008 and 2011, there were 15 163 prelabour repeat caesarean sections among low-risk women giving birth in NSW public hospitals. This represented 5.3% of all births and 19.5% of all caesareans in public hospitals in this period. Of the 61 public hospitals, 40 (65.6%) were regional, and 33 (54.1%) provided primary or secondary obstetric training. Overall, 34.7% of low-risk prelabour repeat caesarean sections occurred before 39 weeks gestation. The low-risk prelabour repeat caesarean section rate decreased from 35.6% in 2008 to 34.1% in 2011.
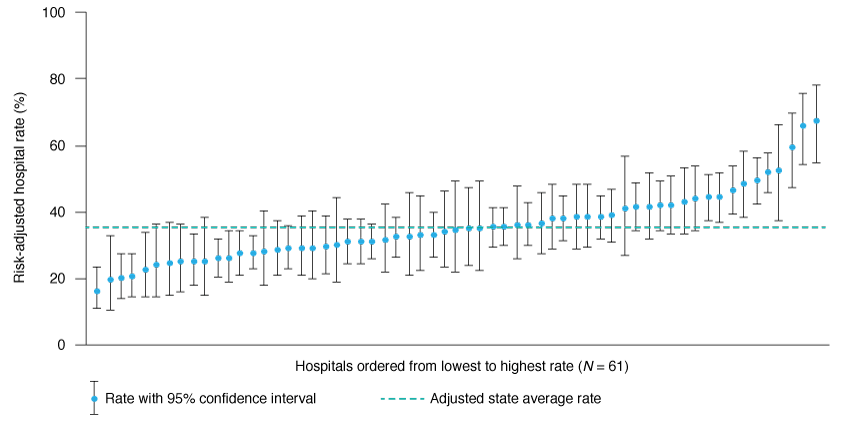
Unadjusted hospital rates of low-risk prelabour repeat caesarean section before 39 weeks gestation varied widely (6.1% to 76.6%). Adjusting for casemix factors increased the between-hospital variation by 4.3%, and adjusting for hospital factors reduced variation by 20.0%. The final adjusted model demonstrated considerable variation (16.3% to 67.5%) in hospital rates of early-term low-risk prelabour repeat caesarean section. Overall, compliance with the NSW policy ranged from 32.5% to 83.7%. Twenty (32.8%) hospitals had an adjusted rate that was significantly different from the adjusted mean of 35.4% (Figure 1).
Smoking (aOR 1.18; 95% CI 1.06, 1.31), private healthcare (aOR 1.77; 95% CI 1.59, 1.96), assisted reproductive technology use (aOR 1.68; 95% CI 1.28, 2.21), two or more previous caesarean sections (aOR 1.70; 95% CI 1.58, 1.83), previous vaginal birth (aOR 1.26; 95% CI 1.14, 1.39), a noncaesarean uterine scar (aOR 2.40; 95% CI 1.48, 3.91) and delivering in a hospital with CPAP facilities (aOR 1.23; 95% CI 1.04, 1.47) were associated with higher odds of early delivery. Having infants that were small for gestational age was associated with lower odds (aOR 0.77; 95% CI 0.65, 0.90) of early delivery. Hospitals with higher rates of low-risk deliveries (aOR 0.69; 95%CI 0.57, 0.82) and higher rates of propensity for vaginal birth after caesarean (aOR 0.96; 95% CI 0.94, 0.98) also had lower odds of early delivery.
Figure 1. Risk-adjusted hospital rates of early (37–38 weeks gestation) low-risk prelabour repeat caesarean section in NSW, 2008–2011 (click to enlarge)
Discussion
The NSW hospital rates of low-risk early-term elective repeat caesarean sections were generally high, with an adjusted average of 35.4%. This rate is similar to a US study that found that 35.8% of early-term elective repeat caesarean sections were performed before 39 weeks gestation.15 One tertiary-level Australian hospital in Queensland reported a rate of low-risk, early-term caesarean section of 59.9%.16 Although this single result is high, it is within the range of hospital early-term caesarean section rates found in the current study (adjusted rates from 16.3% to 67.5%) and also similar to rates in some Canadian hospitals.17
Although other studies have not presented analyses adjusted for casemix and hospital factors, they do report that differences in the rates of elective repeat caesarean sections at early term are major contributors to widely varying overall-term caesarean section rates, ranging from 29% to 57%.18,19 For this study, despite adjustment for casemix and hospital characteristics, we found persistent, large between-hospital variation in rates of early-term repeat caesarean section, suggesting that nonmedical factors are related to the timing of low-risk, prelabour caesarean section. Patients’ preferences and physicians’ decision making vary, and may explain the remaining variation.20 Another contributing factor may be the challenge of scheduling, which may be logistically difficult for hospitals and women19, particularly where travel distance to the hospital is long, such as in rural Australian communities. An Australian population cohort study found that, among low-risk women, 8.5% of caesarean sections planned for 39 weeks gestation resulted in an unscheduled caesarean section due to spontaneous labour before 39 weeks.21 However, a secondary analysis of a randomised controlled trial found that scheduling a planned caesarean section after 39 weeks gestation led to a 60% increase in unscheduled caesarean sections, and a 70% increase in after-hours deliveries. Such findings have financial and resource implications for hospitals.19
Our findings suggest generally poor compliance with the NSW Ministry of Health policy directive concerning the timing of elective repeat caesarean sections across NSW public hospitals. Adjusted rates of compliance across NSW ranged from 32.5% to 83.7%. Although it would be unrealistic to assume that all patient care episodes can comply with guidelines, it is unclear what an acceptable compliance rate would be. One study suggests that 5% of elective caesarean sections before 39 weeks would be acceptable22, while another considers that 30% of elective deliveries before 39 weeks is an achievable quality improvement goal, while recognising that the rate should ultimately be lower.17
Internationally, there has been a concerted effort to reduce the rate of early-term elective caesarean sections, and this rate is one of the maternity quality metrics used in the US.23 Different approaches to reducing the rate of early-term elective caesarean sections have seen varying levels of success24,25 with the ‘hard stop’ approach (enforceable prohibition of elective caesarean sections before 39 weeks) being more effective than other approaches.22 Importantly, reducing elective caesarean sections before 39 weeks gestation has been associated with a reduction in neonatal morbidity.22 For NSW, despite state5 and national2 guidelines recommending elective low-risk caesarean sections at or beyond 39 weeks gestation, large variation in hospital rates for the timing of elective low-risk caesarean section suggests that many NSW hospitals (and possibly hospitals in other Australian states) would benefit from the experience of our international colleagues.
Despite comprehensive, validated population data5, this analysis is limited by the availability of clinical information. Reporting practices between hospitals may differ, and confounding by unmeasured clinical and nonmedical factors is possible. Lack of data on elective repeat caesarean section before 2007 precluded looking for differences before and after introduction of the policy.
Conclusion
There appears to be generally poor compliance with the policy for low-risk prelabour caesarean section from 39 weeks gestation in NSW public hospitals. Large between-hospital variation persisted following adjustment, suggesting that nonmedical factors are related to timing of low-risk prelabour repeat caesarean section. Further strategies, such as those implemented internationally, are required to improve adherence to this evidence based policy.
Acknowledgements
We thank the NSW Ministry of Health for access to the population health data and the Centre for Health Record Linkage for linkage of the datasets. This work was completed while KS was a trainee on the Biostatistics Training Program funded by the NSW Ministry of Health. She undertook this work while based at the Kolling Institute of Medical Research. JF is supported by an Australian Research Council Future Fellowship (FT12010069), and CR by a National Health and Medical Research Council Senior Research Fellowship (1021028).
Copyright:

© 2016 Schemann et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. American College of Obstetricians and Gynecologists. ACOG committee opinion no. 561: nonmedically indicated early-term deliveries. Obstet Gynecol. 2013;121(4):911−5. CrossRef | PubMed
- 2. Royal Australian and New Zealand College of Obsetricians and Gynaecologists. Timing of elective caesarean section at term. Sydney: RANZCOG; 2014 [cited 2015 Oct 15]. Available from: www.ranzcog.edu.au/doc/timing-of-elective-cs-at-term.html
- 3. National Institute for Health and Clinical Excellence. Caesarean section: NICE guidelines [CG132]. Manchester: NICE; 2011 [cited 2015 Oct 15]. Available from: www.nice.org.uk/guidance/cg132
- 4. Morris JM, Algert CS, Falster MO, Ford JB, Kinnear A, Nicholl MC, Roberts CL. Trends in planned early birth: a population-based study. Am J Obstet Gynecol. 2012;207(3):186.e1−8. CrossRef | PubMed
- 5. NSW Health. Maternity − timing of elective or pre-labour caesarean section. Sydney: NSW Health; 2007 [cited 2015 Oct 15]. Available from: www0.health.nsw.gov.au/policies/pd/2007/pdf/PD2007_024.pdf
- 6. Nassar N, Schiff M, Roberts CL. Trends in the distribution of gestational age and contribution of planned births in New South Wales, Australia. PLoS One. 2013;8(2):e56238. CrossRef | PubMed
- 7. Centre for Health Record Linkage. Sydney: NSW Ministry of Health. Quality assurance; 2011 [cited 2015 May 1]; [about 3 screens]. Available from: www.cherel.org.au/quality-assurance
- 8. Bentley JP, Ford JB, Taylor LK, Irvine KA, Roberts CL. Investigating linkage rates among probabilistically linked birth and hospitalization records. BMC Med Res Methodol. 2012;12:149. CrossRef | PubMed
- 9. Schemann K, Patterson JA, Nippita TA, Ford JB, Roberts CL. Variation in hospital caesarean section rates for women with at least one previous caesarean section: a population based cohort study. BMC Pregnancy Childbirth. 2015;15:179. CrossRef | PubMed
- 10. Nippita TA, Schemann K, Roberts CL. Prevalence of noncaesarean uterine surgical scars in a maternity population. Aust N Z J Obstet Gynaecol. 2015 Jul 29. doi: 10.1111/ajo.12357. [Epub ahead of print]. CrossRef
- 11. Nippita TA, Lee YY, Patterson JA, Ford J, Morris JM, Nicholl MC, Roberts CL. Variation in hospital caesarean section rates and obstetric outcomes among nulliparae at term: a population-based cohort study. BJOG. 2015;122(5):702−11. CrossRef | PubMed
- 12. Chen JS, Roberts CL, Simpson JM, Ford JB. Use of hospitalisation history (lookback) to determine prevalence of chronic diseases: impact on modelling of risk factors for haemorrhage in pregnancy. BMC Med Res Methodol. 2011;11:68. CrossRef | PubMed
- 13. Roberts CL, Bell JC, Ford JB, Morris JM. Monitoring the quality of maternity care: how well are labour and delivery events reported in population health data? Paediatr Perinat Epidemiol. 2009;23(2):144−52. CrossRef | PubMed
- 14. Taylor L, Pym M, Bajuk B, Sutton L, Travis S, Banks C. Part 8: validation study NSW midwives data collection 1998. N S W Public Health Bull. 2000;Suppl 11(1):97−9. Available from: www.phrp.com.au/issues/volume-11-issue-1/part-8-validation-study-nsw-midwives-data-collection-1998/
- 15. Tita AT, Landon MB, Spong CY, Lai Y, Leveno KJ, Varner MW, et al. Timing of elective repeat cesarean delivery at term and neonatal outcomes. N Engl J Med. 2009;360(2):111−20. CrossRef | PubMed
- 16. Doan E, Gibbons K, Tudehope D. The timing of elective caesarean deliveries and early neonatal outcomes in singleton infants born 37−41 weeks' gestation. Aust N Z J Obstet Gynaecol. 2014;54(4):340−7. CrossRef | PubMed
- 17. Dunn S, Sprague AE, Fell DB, Dy J, Harrold J, Lamontagne B, Walker M. The use of a quality indicator to reduce elective repeat caesarean section for low-risk women before 39 weeks' gestation: the Eastern Ontario experience. J Obstet Gynaecol Can. 2013;35(4):306−16. CrossRef | PubMed
- 18. Gurol-Urganci I, Cromwell DA, Edozien LC, Onwere C, Mahmood TA, van der Meulen JH. The timing of elective caesarean delivery between 2000 and 2009 in England. BMC Pregnancy Childbirth. 2011;11:43. CrossRef | PubMed
- 19. Glavind J, Henriksen TB, Kindberg SF, Uldbjerg N. Randomised trial of planned caesarean section prior to versus after 39 weeks: unscheduled deliveries and facility logistics − a secondary analysis. PLoS One. 2013;8(12):e84744. CrossRef | PubMed
- 20. Kaimal AJ, Kuppermann M. Understanding risk, patient and provider preferences, and obstetrical decision making: approach to delivery after cesarean. Semin Perinatol. 2010;34(5):331−6. CrossRef | PubMed
- 21. Roberts CL, Nicholl MC, Algert CS, Ford JB, Morris JM, Chen JS. Rate of spontaneous onset of labour before planned repeat caesarean section at term. BMC Pregnancy Childbirth. 2014;14:125. CrossRef | PubMed
- 22. Clark SL, Frye DR, Meyers JA, Belfort MA, Dildy GA, Kofford S, et al. Reduction in elective delivery at <39 weeks of gestation: comparative effectiveness of 3 approaches to change and the impact on neonatal intensive care admission and stillbirth. Am J Obstet Gynecol. 2010;203(5):449.e1−6. CrossRef | PubMed
- 23. The National Quality Forum. Perinatal care (PC) elective delivery. Washington, DC: National Quality Forum; 2011 [updated 2014 May 1] [cited 2015 Oct 15] [about 4 screens]. Available from: manual.jointcommission.org/releases/TJC2015A1/MIF0166.html
- 24. Oshiro BT, Kowalewski L, Sappenfield W, Alter CC, Bettegowda VR, Russell R, et al. A multistate quality improvement program to decrease elective deliveries before 39 weeks of gestation. Obstet Gynecol. 2013;121(5):1025−31. CrossRef | PubMed
- 25. Little SE, Robinson JN, Puopolo KM, Mukhopadhyay S, Wilkins-Haug LE, Acker DA, Zera CA. The effect of obstetric practice change to reduce early term delivery on perinatal outcome. J Perinatol. 2014 Mar;34(3):176−80. CrossRef | PubMed