Abstract
Smoking remains the most preventable cause of early mortality and ill health in Aboriginal people. The Aboriginal Health & Medical Research Council of New South Wales has developed the Aboriginal Tobacco Resistance and Control (ATRAC) Yarning Tool with a range of key stakeholders, to contribute to reducing the prevalence of smoking in Aboriginal communities.
The Yarning Tool was adapted from the ATRAC Framework and aims to promote the meaningful discussion, planning and strengthening of tobacco resistance and control activities using a continuous quality improvement (CQI) approach. CQI provides an opportunity to closer align current health service practice with evidence.
The Yarning Tool was piloted using focus group testing across four Aboriginal Community Controlled Health Services (ACCHSs) and three Local Health Districts. Purposive sampling was used to ensure that services engaged were from a diverse range of settings, with representation from metropolitan, regional and rural areas, and services with varying degrees of tobacco control capacity.
Overall, feedback on the Yarning Tool and its potential use was positive. Pilot participants consistently reported that the Yarning Tool brought staff from a range of positions together to focus on tackling tobacco for the service and community. The pilot participants agreed that the Yarning Tool could be practical for the planning and reviewing stages of a CQI activity, and recommended that the tool should be completed every 6 months.
The Yarning Tool is a simple tool to guide the ATRAC Framework principles into practice, and provides a platform to support Aboriginal community-led efforts, and coordination and integration of tobacco control efforts. The tool shows promise as a mechanism to encourage ACCHSs and other relevant services to use a CQI approach to reduce tobacco use in Aboriginal communities.
Full text
Setting the scene
Aboriginal tobacco resistance and control in NSW, Australia
Smoking remains the most preventable cause of poor health and early death among Aboriginal people in Australia, despite 30% of Aboriginal people having never smoked.1,2 In New South Wales (NSW), Aboriginal people are twice as likely to smoke compared with the general population3, resulting in a range of serious negative health consequences and inequities. Reducing smoking prevalence and exposure to second-hand smoke is therefore vital to improving the life expectancy and health of Aboriginal people in NSW.4
The Aboriginal Health & Medical Research Council of NSW (AH&MRC) has developed, delivered and evaluated culturally appropriate programs and resources in tobacco resistance and control under the AH&MRC Tobacco Resistance and Control (A-TRAC) Program since 2009. These have included community education resources, staff training and professional development, and social media campaigns. In 2015, the AH&MRC and NSW Ministry of Health released the Aboriginal Tobacco Resistance and Control (ATRAC) Framework: a strategic framework for Aboriginal tobacco resistance and control in NSW to help guide the efforts of those working in Aboriginal tobacco resistance and control in NSW.5 The ATRAC Framework was developed with wide consultation and complements other important strategic directions, such as the NSW Tobacco Strategy 2012–2017.5
The ATRAC Framework identifies relevant evidence, key principles and best-practice approaches for reducing Aboriginal smoking and tobacco-associated harm in NSW.6 The framework informs decision making about resource allocation, planning, implementation, and the evaluation of existing and future Aboriginal tobacco resistance and control activities at local, regional and state levels. After the release of the ATRAC Framework, the ATRAC Subcommittee identified a need for supporting tools and resources to improve the implementation and integration of the ATRAC Framework in practice. This subcommittee was established in 2012 to oversee and facilitate the use of the ATRAC Framework. The subcommittee is represented by key stakeholders involved in tobacco control in NSW, including Aboriginal Community Controlled Health Services (ACCHSs), and government and nongovernment organisations.
Using a continuous quality improvement approach for ATRAC
Continuous quality improvement (CQI) is a “system of regular reflection and refinement to improve processes and outcomes that can lead to quality health care”, and can have an important role in planning and reviewing tobacco resistance and control in health services.7 It has previously been suggested that a national CQI framework can contribute to closing the gap, a strategy that aims to nationally reduce Indigenous disadvantage with respect to life expectancy and health outcomes.7,8 A CQI approach provides the potential to align current practice more closely with evidence to strengthen tobacco resistance and control by directly focusing efforts to achieve best practice.9,10 In particular, the Plan, Do, Study, Act (PDSA) cycle, where activities are planned, implemented, evaluated and modified, can be harnessed to strengthen tobacco control efforts, as well as increase staff enthusiasm for CQI activities.7,9
ACCHSs have a longstanding interest in using CQI processes in their health services, including the PDSA cycle.7 On top of the practical component of service improvement that CQI can provide, some funding agreements offered by the Australian Government Department of Health have a requirement for all services funded under the Primary Health Care Services Activity to embed a robust CQI approach across service delivery and business practice.11 However, there are limited examples of tobacco resistance and control tools or resources that use a comprehensive CQI approach.
To achieve maximum benefits and value for money, efforts to address Aboriginal smoking need to be evidence based, coordinated, integrated, reviewed and adjusted if required.6 These factors, along with recommendations from the ATRAC Framework Subcommittee, have been the drivers for the AH&MRC to collaborate with a range of stakeholders to develop a specific tool to support the implementation of the ATRAC Framework using CQI approaches. Although this tool has been developed with a focus on use in ACCHSs, it is envisaged that all those working in Aboriginal tobacco control in NSW will be able to use the tool in conjunction with the ATRAC Framework.
The ATRAC Framework Yarning Tool
Development of the tool
The terms ‘yarn’ and ‘yarning’ are used by Aboriginal peoples in everyday language, referring to a process and exchange in which respect, protocol and engagement in individuals’ relationships are offered in a culturally safe environment.12 Yarning has previously been described as a valuable process in action research and resource development to facilitate the development of tobacco control policies.12,13 This process can empower staff to create policy change that not only affects their own health, but also the health of others around the Aboriginal organisation for which they work.12 As successful tobacco resistance and control activities often require empowerment, engagement and ownership at multiple levels14, a specialised yarning tool can be a culturally appropriate process to foster these elements to tackle tobacco in Aboriginal communities and health services.
The ATRAC Framework Yarning Tool was developed to promote meaningful discussion and planning of ATRAC activities using a CQI approach. The Yarning Tool was adapted from, and highlights, the six action areas of the ATRAC Framework: leadership, partnerships and coordination; community action awareness and engagement; workforce development; supportive environments; quitting support; and evidence evaluation and research.5 The Yarning Tool contains yarning topics that have been guided by the recommended actions under each of the six action areas, and enables planning and accountability for any services aiming to strengthen Aboriginal tobacco resistance and control. An overview of the Yarning Tool and the ATRAC Framework is shown in Figure 1; the complete Yarning Tool can be found on the AH&MRC website.15
Figure 1. ATRAC Framework Yarning Tool overview
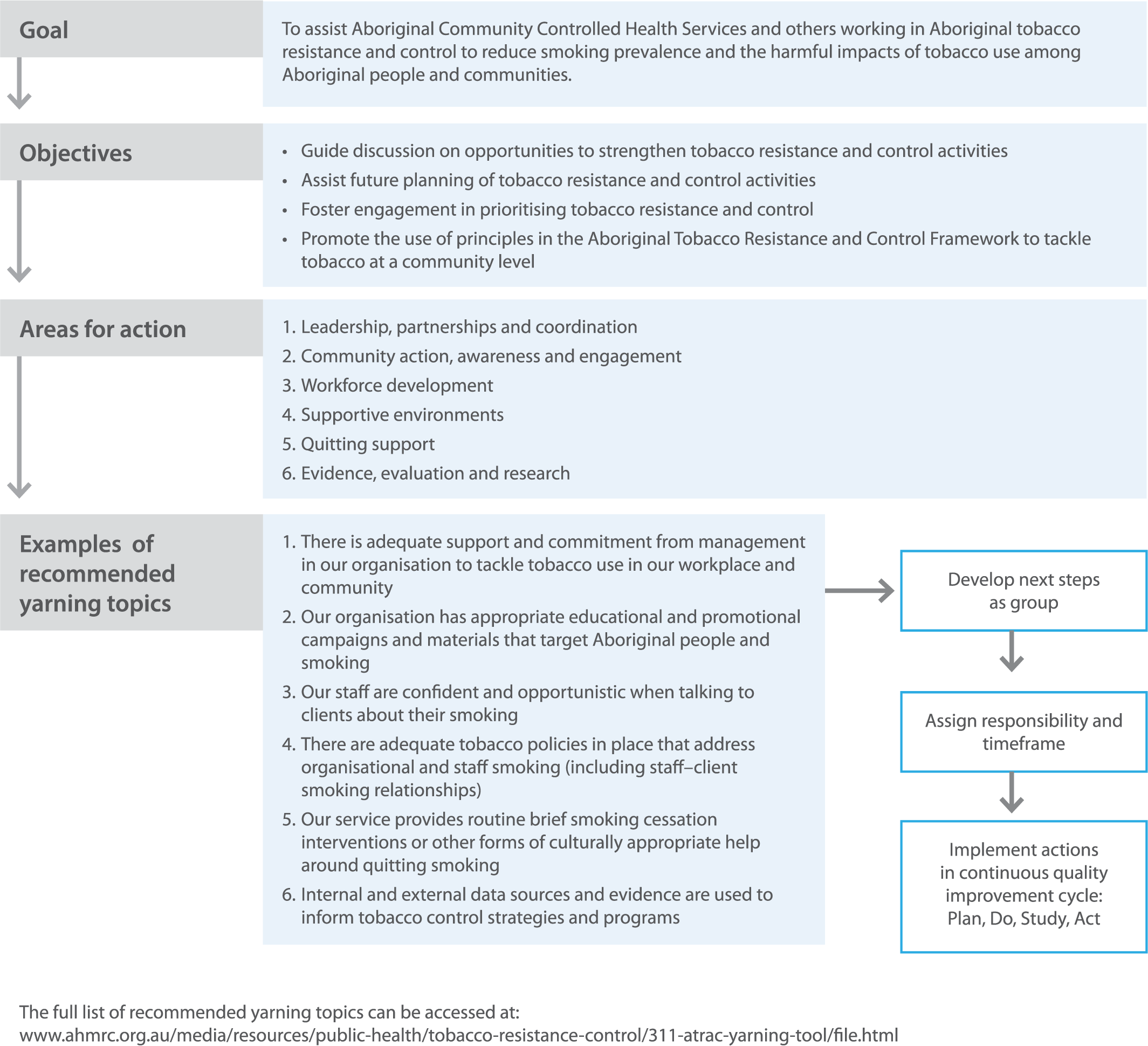
The Yarning Tool takes approximately 60 minutes to complete.15 It is suggested that the tool is completed by teams working as a group with a facilitator, to encourage discussion on different perceptions of current tobacco resistance and control activities and future directions in this area.15
Piloting the Yarning Tool
The Yarning Tool was piloted across four ACCHSs and three Local Health Districts (LHDs). Purposive sampling was used to ensure that services engaged were from a diverse range of settings, with representation from metropolitan, regional and rural areas, and services with varying degrees of tobacco control capacity.
Each piloting session consisted of participating staff completing the Yarning Tool, with face-to-face facilitation from A-TRAC Program staff, using a focus group format. In an attempt to maximise trust and authenticity, participants were given the option of completing the piloting session without A-TRAC Program staff present. Targeted questions were asked at the end of each piloting session to guide discussion into how the Yarning Tool could be linked to CQI activities; the tool’s usability, further uses and format; and general comments for improvement. Participant responses were recorded using handwritten notes and analysed by A-TRAC Program staff. Consistent responses to the targeted questions were grouped together and discussed by A-TRAC Program staff to further develop and refine the Yarning Tool.
Results from piloting
In total, four ACCHSs piloted the Yarning Tool after a targeted expression-of-interest process. All services that expressed interest were included in the pilot, except one service because of scheduling. An additional three LHDs piloted the Yarning Tool at a clinical nicotine replacement therapy workshop hosted by the AH&MRC. Participants from LHDs only completed parts of the Yarning Tool that they found relevant and provided feedback about the potential of the tool in their workplace setting.
Participating ACCHSs and LHDs varied in terms of geographic location, remoteness and level of tobacco control activity. Only one ACCHS that participated in the piloting had a dedicated Tackling Tobacco Team. Participants came from a broad range of service positions, including health promotion workers, alcohol and other drug workers, dentists, Aboriginal health workers, practice managers and tobacco action workers. All participating staff opted to have piloting sessions facilitated by A-TRAC Program staff.
Overall, feedback on the Yarning Tool and its potential use was positive. Pilot participants consistently reported that the tool brought staff from a range of positions together to focus on tackling tobacco for the individual service and community. The A-TRAC Program staff also observed during the piloting of the Yarning Tool that staff perceptions were not always aligned with each other. For example, one nonclinical staff member stated that an action from the tool was currently being achieved, but another clinical colleague was unaware of this.
Participants also noted that the Yarning Tool helped to reduce the traditional division of clinical and nonclinical staff that is experienced in smoking cessation. The tool allowed staff to reflect on their achievements collectively while exploring future action. The participants agreed that the Yarning Tool could be practical for the planning and reviewing stages of a CQI activity, and recommended that it should be completed every 6 months. Participants commented that the tool is particularly relevant for the Plan and Study components of the PDSA cycle, because it can assist planning and document progress of implemented tobacco control and resistant activities that services adopt.
Constructive feedback from the pilot was used by the A-TRAC Program staff to further adjust and strengthen the Yarning Tool. For example, the tool was initially designed as a self-assessment tool to support the grading and tracking of service performance around tobacco control and resistance activities over time. However, feedback after the first pilot session suggested that standardisation of such activities would require further research and evidence and that, instead, a Yarning Tool could be an effective tool for supporting CQI in the meantime. Participants also recommended later that the Yarning Tool contain more opportunities to document current activities so it can better assist staff to reflect on achievements and identify potential future tobacco control activities. In response, the tool was modified to contain a section where copies of relevant documents could be stored to ensure sufficient documentation is provided.
One participant noted that it was particularly challenging to engage all relevant staff to collectively use the Yarning Tool, particularly clinical staff. However, the participant then stated that there was a section in the Yarning Tool around organisational support that can be implemented in a PDSA cycle, if required.
Conclusion and next steps
The AH&MRC is committed to supporting NSW ACCHSs to strengthen tobacco resistance and control for Aboriginal communities. The Yarning Tool provides a mechanism to support the coordination and integration of Aboriginal tobacco resistance and control efforts by guiding the ATRAC Framework principles into practice. In particular, the Yarning Tool can assist ACCHSs and other relevant services to use a CQI approach to reduce the prevalence of tobacco use in Aboriginal communities.
The Yarning Tool will be made widely available to ACCHSs and other relevant services, and promoted as a method to encourage the discussion and planning of tobacco control and resistance activities. It will also be integrated into training opportunities provided by the A-TRAC Program. In addition, the Yarning Tool can be used outside this context (see instructions in the published version of the tool).
It is hoped that the Yarning Tool can be used as a foundation to develop future tobacco resistance and control standards for those working to address tobacco-related harm in Aboriginal communities.
Acknowledgements
The authors acknowledge Dr Jennifer Hunt for her input into the paper, and staff from the ACCHSs and LHDs that participated in the piloting of the Yarning Tool. This work was completed while Alvin Lee was employed as a trainee in the NSW Public Health Training Program funded by the NSW Ministry of Health. He undertook this work while based at the AH&MRC.
Copyright:

© 2016 Lee et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Centre for Epidemiology and Evidence. The health of Aboriginal people of NSW: report of the Chief Health Officer 2012. Sydney: NSW Ministry of Health; 2012 [cited 2016 Oct 16]. Available from: www.health.nsw.gov.au/epidemiology/Publications/Aboriginal-Health-CHO-report.pdf
- 2. Vos T, Barker B, Begg S, Stanley L, Lopez AD. Burden of disease and injury in Aboriginal and Torres Strait Islander people: the Indigenous health gap. Int J Epidemiol. 2009;38(2):470–7. CrossRef | PubMed
- 3. Centre for Epidemiology and Evidence. Health Stats NSW: current smoking in adults. Sydney: NSW Ministry of Health; 2016 [cited 2016 Oct 16]. Available from: www.healthstats.nsw.gov.au/Indicator/beh_smo_age/beh_smo_atsi
- 4. Intergovernmental Committee on Drugs. National tobacco strategy 2012–2018. Canberra: Commonwealth of Australia; 2012 [cited 2016 Oct 16]. Available from: www.nationaldrugstrategy.gov.au/internet/drugstrategy/publishing.nsf/content/D4E3727950BDBAE4CA257AE70003730C/$File/National%20Tobacco%20Strategy%202012-2018.pdf
- 5. Aboriginal Health & Medical Research Council of NSW, NSW Ministry of Health. The ATRAC ramework: a strategic framework for Aboriginal tobacco resistance and control in NSW. Sydney: AH&MRC and NSW Ministry of Health; 2014 [cited 2016 Oct 16]. Available from: www.health.nsw.gov.au/tobacco/Publications/atrac-framework.pdf
- 6. Sarin J, Hunt K, Ivers R, Smyth C. Lifting the burden: a coordinated approach to action on Aboriginal tobacco resistance and control in NSW. Public Health Res Pract. 2015;25(3):e2531528. CrossRef | PubMed
- 7. Wise M, Angus S, Harris E, Parker S. National appraisal of continuous quality improvement initiatives in Aboriginal and Torres Strait Islander primary health care. Melbourne: The Lowitja Institute; 2013 [cited 2016 Oct 16]. Available from: www.lowitja.org.au/sites/default/files/docs/National-Appraisal-of-CQI-FINAL.pdf
- 8. Schierhout G, Brands J, Bailie R. Audit and best practice for chronic disease extension project 2005–2009: final report. Melbourne: The Lowitja Institute; 2010 [cited 2016 Oct 16]. Available from: www.lowitja.org.au/sites/default/files/docs/ABCDE_Report2011.pdf
- 9. Bailie S, Dowden C, Burke P, Brown A, Weeramanthri T, Thompson S, et al. Variation in quality of preventive care for well adults in Indigenous community health centres in Australia. BMC Health Serv Res. 2011;11(1):139. CrossRef | PubMed
- 10. Ford DR, Knight A. The Australian primary care collaboratives: an Australian general practice success story. Med J Aust. 2010;193(2):90–1. PubMed
- 11. Australian Government Department of Health. Department of Health. Canberra: Commonwealth of Australia; 2016. Aboriginal and Torres Strait Islander Health – primary health funded activities; 2016 [cited 2016 Oct 16]. [about 3 screens] Available from: www.health.gov.au/internet/main/publishing.nsf/Content/indigenous-primary-health-care-lp
- 12. Fredericks BL, Adams K, Finlay SM, Fletcher G, Andy S, Briggs L, et al. Engaging the practice of yarning in action research. Action Learning and Action Research Journal. 2011;17(2):7–19. Article
- 13. Martin KL. Please knock before you enter: Aboriginal regulation of outsiders and the implications for researchers. Teneriffe, Queensland: Post Pressed; 2008.
- 14. Ivers R. Indigenous Australians and tobacco: a literature review. Darwin: Menzies School of Health Research, Cooperative Research Centre for Aboriginal and Tropical Health; 2001 [cited 2016 Oct 16]. Available from: www.lowitja.org.au/sites/default/files/docs/Indigenous_Australians_and_Tobacco.pdf
- 15. Aboriginal Health & Medical Research Council of NSW. The ATRAC yarning tool: where are we in tackling tobacco in our service and for our mob? Sydney: AH&MRC; 2016. [cited 2016 Oct 16] Available from: www.ahmrc.org.au/media/resources/public-health/tobacco-resistance-control/311-atrac-yarning-tool/file.html