Abstract
Objectives: The Health Star Rating (HSR) system is an interpretative front-of-pack labelling (FOPL) scheme for Australia and New Zealand, which aims to guide consumers towards foods higher in components associated with a healthy diet and lower in energy and nutrients associated with an increased risk of disease, and thereby reduce the diet-related burden of disease.
Type of program: A government-endorsed and funded nutrient profiling model for application to packaged foods and beverages in retail environments.
Methods: By considering the nutritional profile of a product, based on widely accepted risk-increasing and beneficial components, and assigning a rating from 0.5 to 5 stars, the HSR system simplifies complex nutrition information and messages to highlight the healthier options within a given product range.
Results: Implementation of the HSR system is progressing well, with a rapidly increasing presence in supermarkets. Consumer understanding and use of the system is increasing and sentiments are generally favourable. People are changing purchasing behaviour by using the system to select healthier choices. The great majority of HSRs displayed on packs are accurate and industry is reformulating products to improve nutritive quality. However, some issues of concern have been raised during the implementation period. These are being investigated through an independent review of the system.
Lessons learnt: The experience of the HSR system, particularly its governance structures, has demonstrated that when disparate stakeholders are included in the process, a workable and acceptable system that achieves tangible outcomes can be implemented.
Full text
Introduction
Front-of-pack labelling (FOPL) is recommended by the World Health Organization as part of a suite of population health measures to improve diets and thereby reduce the diet-related burden of disease, particularly for children.1 Appropriately designed and targeted FOPL is seen to be an effective way to guide consumers towards options lower in components associated with an increased risk of disease.2 FOPL also has the potential to provide incentives for food manufacturers to reformulate products to improve the nutritional quality of the food supply.3
The HSR system is a government-endorsed interpretative FOPL scheme for Australia and New Zealand. It assesses the nutritional profile of packaged foods, based on widely accepted risk-increasing and beneficial components, and assigns a rating from 0.5 to 5 stars. The system provides an accessible, standardised way to compare similar packaged products at point of sale, simplifying complex nutrition information and messages to highlight the healthier options.
The overarching objective of the HSR system is “to provide convenient, relevant and readily understood nutrition information and/or guidance on food packs to assist consumers with making informed food purchases and healthier eating choices”.4
As outlined in a perspective paper in this issue, there has been criticism of the HSR system.5 It is important to note that the system was designed to support and not replace general dietary guidance, as provided by the Australian Dietary Guidelines (ADG) and New Zealand Eating and Activity Guidelines. Neither does it provide messaging around healthy eating patterns in general (e.g. serving sizes, consumption frequencies). Dietary guidance should help inform what goes on the shopping list while the HSR system guides choices between similar products at point of purchase.
Development and governance of the Health Star Rating (HSR) system
FOPL has a long and often controversial history. In Australia and New Zealand, development started in 2004 when Australian federal, state and territory and New Zealand government ministers responsible for food regulation first considered the UK ‘traffic light’ approach to FOPL. In 2009, the responsible ministers endorsed an FOPL Policy Statement which stated that an FOPL scheme should guide consumer choice, be consistent with other health strategies and affect the environment in which consumers make choices.6 However, conflicting views among stakeholders inhibited further development.
The impasse was overcome in 2012 when ministers endorsed a recommendation from a review of food labelling law and policy7 that an interpretative FOPL system be developed that reflected a comprehensive nutrition policy and agreed public health priorities. A collaboration between national, state and territory governments, along with food industry and public health and consumer groups, was established to develop the system. The process was consultative, drew on a broad range of expertise, and collected and commissioned evidence to support recommendations.
Implementation of the system started in June 2014 and is overseen by an HSR Advisory Committee comprising stakeholders from government, industry, and consumer and public health organisations. Ministers also agreed that the system would be based on economic analysis and advice, be voluntary, and that uptake and success would be reviewed after 5 years. The administration of the HSR system is wholly funded by the Australian federal, state and territory and New Zealand governments. For industry, the only costs associated with using the HSR are costs of calculating the HSR for their products and associated labelling changes; there is no fee to use the system.
HSR Calculator and algorithm
The HSR system is underpinned by the HSR Calculator, a modified version of the Nutrient Profiling Scoring Criterion8 developed by Food Standards Australia New Zealand for the regulation of health claims on food. The algorithm driving the HSR Calculator is a nutrient profiling model that assesses certain ‘negative’ components of public health concern (energy, saturated fat, sodium and total sugars) and ‘positive’ components (fibre, protein, and fruit, vegetable, nut and legume content) to produce a summary score. Scores are then scaled according to HSR category (Table 1)9 and converted into a rating.
Table 1. HSR categories
| Category | Definition |
| 1 | Beverages other than dairy beverages |
| 1D | Dairy beverages |
| 2 | All foods other than those included in Category 1, 1D, 2D, 3 or 3D |
| 2D | Dairy foods other than those included in Category 1D or 3D |
| 3 | Oils and spreads, defined as follows:
|
| 3D | Cheese and processed cheese as defined in Standard 2.5.4 (with calcium content >320 mg/100 g) |
A distinctive feature of the system is that HSR categories are scaled with the intention of creating a range of scores within any given product category to allow differentiation between similar products. This is a key function of the HSR system – to allow ready comparisons within product ranges and enable the identification of healthier options; for example, to compare an intensely sugar-sweetened, ‘low-fat’ yoghurt to unsweetened yoghurt containing freeze-dried strawberries, rather than to strawberry-flavoured liquorice.
System performance
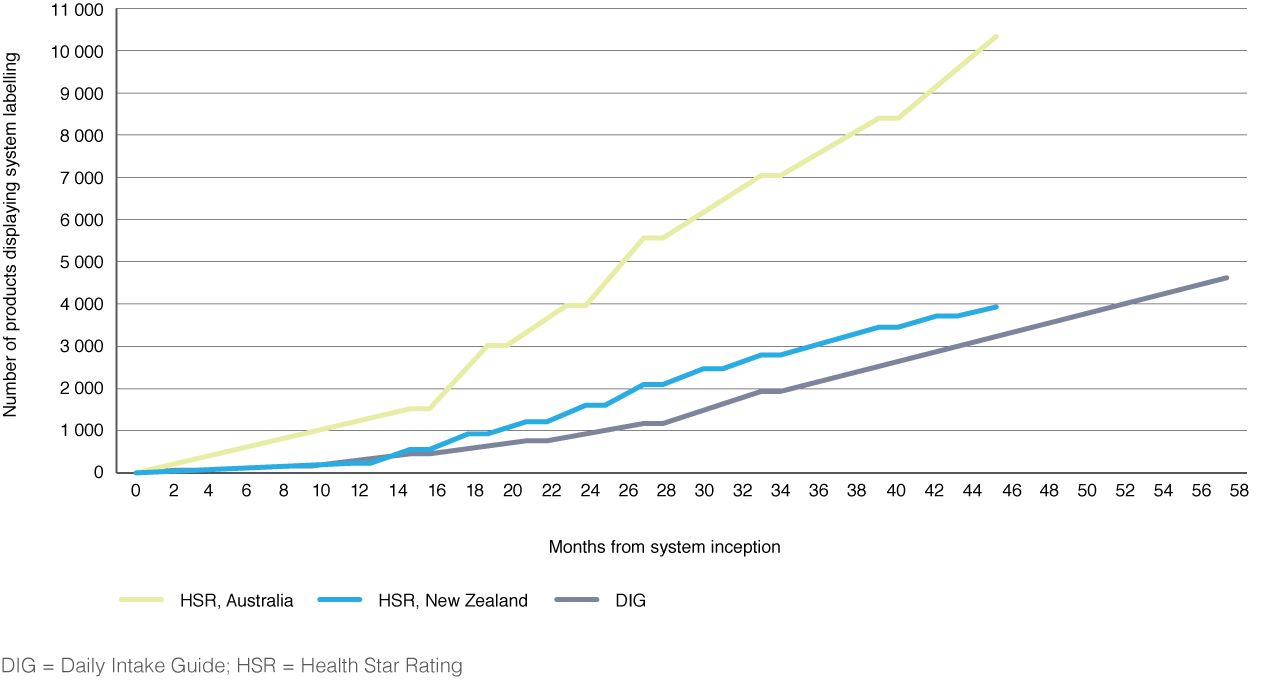
Voluntary industry uptake of HSR has been strong, particularly when benchmarked against the Daily Intake Guide FOPL system which has been in place in Australia for several years (Figure 1). As of March 2018, about 10 300 products in Australian supermarkets have displayed the HSR graphic, representing a commitment by more than 160 companies10, and over 3900 products bore the HSR label in New Zealand.11
Figure 1. Comparison of uptake of the Daily Intake Guide and Health Star Rating systems in Australia and New Zealand (click to expand)
The National Heart Foundation of Australia monitors and reports on uptake, compliance with system guidance, and consumer use and understanding of the system in Australia. The evidence shows that companies are applying HSRs with high fidelity: the most recent assessment of displayed HSRs against calculated HSRs found that 92% were accurate12 according to current system guidance, and, of those that were not accurate, almost two-thirds (64%) had understated HSRs.
Monitoring of consumer awareness, attitudes and interaction with the HSR system also points to improvements in how people understand and use the system over time and as more products adopt the label. The most recent assessment13 found that 84% of respondents were aware of the HSR system. Of these, a majority believed it to be easy to use (76%) and understand (76%) and said it made choosing products easier (63%). Two-thirds (66%) reported that their confidence in the system was high or somewhat high and more than two-thirds (71%) agreed that the system helped consumers identify healthier options within the same food category. Two-thirds (67%) reported that the system influenced purchasing decisions when shopping and, of these, nearly 88% stated that they would continue to purchase this product. Results also demonstrated the power of advertising: for consumers that recall HSR marketing, 75% were influenced to buy a different product.
High levels of consumer understanding of the HSR system have been supported by independent research comparing FOPL systems. This has found that the HSR system performed better than either the Daily Intake Guide or multiple traffic light systems on consumers’ food choices and willingness to pay14, and on discrimination between ‘healthy’ and ‘unhealthy’ foods.15 Another study indicated that, among regular users of nutrition labels, the HSR system prompted healthier food choices than the sole use of the Nutrition Information Panel.16
There are numerous anecdotal reports of companies reformulating products to achieve higher HSRs by reducing sugar, fat and/or salt, and increasing fibre. Early published research is beginning to confirm this, reporting that food manufacturers and retailers are reformulating products to reduce negative and increase positive nutritive components, and that this change is greater for products displaying an HSR.3,17
There has been some controversy about how the HSR system scores five-food-group (FFG) foods (commonly known as ‘core’ foods) and ‘discretionary’ foods, as referred to in the ADG (noting that the New Zealand Eating and Activity Guidelines do not have a similar binary distinction). However, studies have found that the HSR system generally discriminates well between FFG and discretionary products. In a NSW study18 comparing the HSR system with the traffic light system used in schools and health facilities, the HSR system outperformed the alternative in discriminating between FFG and discretionary foods. This study also found that only 14% of discretionary products scored 3.5 stars or more. These ‘outliers’ may indicate a need for refinement of the system, although many of these products may indeed be considered objectively ‘more healthy’ than their ‘discretionary’ classification would suggest (i.e. lower in negative components and/or higher in positive components). On the other hand, 21% of FFG products scored fewer than 3.5 stars, possibly reflecting higher levels of the negative components than expected for FFG products.
In a separate study, Jones et al.19 concluded that while HSRs for 13.4% of products did not appear to align with dietary guidance based on their a priori categorisation, after an assessment of the actual nutrient content of products identified as outliers, only 17% (2% overall) were considered to be true failures of the HSR system. They reported that this indicated “the scope of genuine misalignment between the ADGs and the HSR algorithm is very small”.
Another study20 has suggested that the HSR undermines the ADG by facilitating the marketing of discretionary products and that there is selective application of HSRs to higher-scoring products by industry. However, from a database of 1269 products in Australia carrying the HSR, the paper also reported that the median number of stars displayed on discretionary foods was 2.5, significantly lower (p < 0.05) than the median of 4 found on core foods.
While the HSR generally ‘nudges’ people in the direction of healthier choices, it is acknowledged that the system cannot perfectly categorise food products along a healthy–not healthy scale; no FOPL scheme can ever truly replace general dietary guidance nor satisfy all demands. Several substantive issues have also arisen during the course of implementation that have attracted criticism of the system and affected consumer trust.
Although the most recent monitoring results13 now indicate that few people have low confidence in the system (e.g. 3% considered it inaccurate or unreliable, 2% thought it misleading, and only 1% thought HSRs could be ‘bought’), there has been substantial negative comment from sectors of the community about specific issues that need to be resolved if trust is to be maintained. Chief among these are the rules permitting products to count nutrients from added ingredients when calculating HSRs – the so-called ‘as prepared’ rules. These include products to which, for example, skim milk, eggs or lean meat are added before consumption. Another major issue is how sugar is reflected in ratings and whether total sugars, added sugars or free sugars should be used in the HSR Calculator. These and other issues are being investigated by the HSR Advisory Committee and in the independent review of the system.
Health Star Rating system review
As required by the Australian and New Zealand Ministerial Forum on Food Regulation when the HSR system was approved, an independent 5-year review of the system is currently under way. A draft review report was published in February 201921, with a final report due to Ministers in mid 2019. The review is considering if, and how well, the objectives of the system have been met and is identifying options for improvements to, and the ongoing implementation of, the system. The review is being undertaken with a full commitment to transparency and accessibility, with multiple consultations held across Australia and in New Zealand. The reviewers have sought the views of a diverse and comprehensive range of stakeholders on issues such as governance, communications and system enhancements.
Conclusion
The overriding public health message for consumers remains to eat according to dietary guidelines. However, when purchasing processed packaged foods, the HSR system supports consumers in making healthier choices. Previously, consumers had to base their choices on marketing and, when well versed, the Nutrition Information Panel and other nutritional information provided on-pack. The HSR provides readily understandable information and an alternative, government-endorsed and robust way to help people select healthier options.
Implementation of the HSR system is progressing well, with a rapidly increasing presence in supermarkets. Monitoring indicates that consumer understanding and use of the system is increasing and sentiments are generally favourable. The available evidence suggests that people are using the system to influence product choice at point of purchase and are changing their long-term purchasing behaviour. The vast majority of HSRs on packs are accurate and industry is reformulating products to reduce levels of risk-associated components and increase positive components. The current 5-year review will further guide progress on the implementation of the system.
The experience of the HSR system, particularly its governance structures, has demonstrated that when disparate stakeholders are included in the process and encouraged to engage ‘in good faith’, a workable and acceptable system that achieves tangible outcomes can be implemented.
Acknowledgements
Thanks to Kate Turner, Julianne Brettargh, Kathleen Orr, Karen Tuckerman and Jessica Down (FOPL Secretariat) for reviewing this paper.
Peer review and provenance
Externally peer reviewed, commissioned.
Copyright:

© 2019 Maganja et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. World Health Organization. Report of the Commission on Ending Childhood Obesity. Implementation plan: executive summary. Geneva: World Health Organization; 2017 [cited 2019 Jan 30]. Available from: www.who.int/end-childhood-obesity/publications/echo-plan-executive-summary/en/
- 2. Cecchini M, Warin L. Impact of food labelling systems on food choices and eating behaviours: a systematic review and meta‐analysis of randomized studies. Obes Rev. 2016;17(3):201–10. CrossRef | PubMed
- 3. Mhurchu CN, Eyles H, Choi YH. Effects of a voluntary front-of-pack nutrition labelling system on packaged food reformulation: the Health Star Rating system in New Zealand. Nutrients. 2017;9(8):E918. CrossRef | PubMed
- 4. Food Regulation. Canberra: Commonwealth of Australia. Project committee objectives and principles; [updated 2016 Nov 21; cited 2018 Mar 8]; [about 4 screens]. Available from: foodregulation.gov.au/internet/fr/publishing.nsf/Content/frontofpackobjectives
- 5. Lawrence M, Pollard CM, Vidgen H, Woods J. The Health Star Rating system – is its reductionist (nutrient) approach a benefit or risk for tackling dietary risk factors? Public Health Res Pract. 2019;29(1):e2911906. CrossRef
- 6. Australia and New Zealand Food Regulation Ministerial Council. Front of pack labelling policy statement. Canberra: Commonwealth of Australia; 2009 [cited 2019 Jan 30]. Available from: foodregulation.gov.au/internet/fr/publishing.nsf/Content/publication-Policy-Statement-on-Front-of-Pack-Labelling
- 7. Blewett N, Goddard N, Pettigrew S, Reynolds C, Yeatman H. Labelling logic: review of food labelling law and policy. Canberra: Commonwealth of Australia; 2011 [cited 2019 Jan 31]. Available from: www.choice.com.au/~/media/9023443697c640adbf014dbbfec52199.ashx?la=en
- 8. Food Standards Australia New Zealand. Canberra: Food Standards Australia New Zealand. Nutrient profiling scoring calculator for standard 1.2.7; [updated 2016 Nov; cited 2018 Mar 12]; [about 2 screens]. Available from: www.foodstandards.gov.au/industry/labelling/pages/nutrientprofilingcalculator/Default.aspx
- 9. Front-of-Pack Labelling Secretariat. Guide for industry to the Health Star Rating Calculator (HSRC), version 6. Canberra: Australian Department of Health; 2018 [cited 2019 Jan 30]. Available from: www.healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/Content/E380CCCA07E1E42FCA257DA500196044/$File/Guide%20for%20Industry%20to%20the%20Health%20Star%20Rating%20Calculator.pdf
- 10. National Heart Foundation of Australia. Report for wave 7 of additional (point-in-time) uptake monitoring of the Health Star Rating (HSR) system, in Australia: February–March 2018. Melbourne: National Heart Foundation of Australia; 2018. p. 28. Available on request from the Front-of-Pack Labelling Secretariat at [email protected]
- 11. Ministry for Primary Industries. Wellington, NZ: Ministry for Primary Industries. Health Star Rating resources; [updated 2018 Apr; cited 2018 Jul 20]. Available from: www.mpi.govt.nz/food-safety/food-safety-for-consumers/food-labelling/health-star-ratings/health-star-rating-resources/
- 12. National Heart Foundation of Australia. Assessment of the Health Star Rating (HSR) displayed on pack against the calculated HSR (sub-section of AOE1) – reporting timeframe: June 2016 to June 2017. Melbourne: National Heart Foundation of Australia; 2017 [cited 2019 Jan 30]. p 21. Available on request from the Front-of-Pack Labelling Secretariat at [email protected]
- 13. National Heart Foundation of Australia. Report on the monitoring of the implementation of the Health Star Rating system: area of enquiry 2 – consumer awareness and ability to use the Health Star Rating system correctly. Melbourne: National Heart Foundation of Australia; 2018 [cited 2019 Jan 20]. p. 64. Available on request from the Front-of-Pack Labelling Secretariat at [email protected]
- 14. Talati Z, Norman R, Pettigrew S, Neal B, Kelly B, Dixon H, et al. The impact of interpretive and reductive front-of-pack labels on food choice and willingness to pay. Int J Behav Nutr Phys Act. 2017;4(171):10. CrossRef | PubMed
- 15. Talati Z, Pettigrew S, Ball K, Hughes C, Kelly B, Neal B, et al. The relative ability of different front-of-pack labels to assist consumers discriminate between healthy, moderately healthy, and unhealthy foods. Food Qual Prefer. 2017;59:109–13. CrossRef
- 16. Mhurchu CN, Volkova E, Jiang Y, Eyles H, Michie J, Neal B, et al. Effects of interpretive nutrition labels on consumer food purchases: the Starlight randomized controlled trial. Am J Clin. 2017;105(3):695–704. CrossRef | PubMed
- 17. Mantilla-Herera AM, Crino M, Erskine HE, Sacks G, Ananthapavan J, Mhurchu CN, Lee YY. Cost-effectiveness of product reformulation in response to the Health Star Rating food labelling system in Australia. Nutrients. 2018;10(5):E614. CrossRef | PubMed
- 18. Dunford E, Cobcroft M, Thomas M, Wu J. Technical report: alignment of NSW healthy food provision policy with the Health Star Rating system. Sydney: NSW Ministry of Health; 2015 [cited 2019 Jan 30]. Available from: www.health.nsw.gov.au/heal/Publications/health-star-rating-system.pdf
- 19. Jones A, Rådholm K, Neal B. Defining ‘unhealthy’: a systematic analysis of alignment between the Australian Dietary Guidelines and the Health Star Rating system. Nutrients. 2018;10(4):E501. CrossRef | PubMed
- 20. Lawrence MA, Dickie S, Woods JL. Do nutrient-based front-of-pack labelling schemes support or undermine food-based dietary guideline recommendations? Lessons from the Australian Health Star Rating System. Nutrients. 2018;10(1):32. CrossRef | PubMed
- 21. Health Star Rating System. Canberra: Commonwealth of Australia; 2014. Public consultation on draft report on the five year review; 2019 Feb 27 [cited 2019 Mar 4]; [about 1 screen]. Available from: healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/Content/news-20190227