Abstract
Objectives: The cancer burden is high among Australia’s Indigenous population. Following a period of increasing attention by researchers, policy makers and consumers, this study aimed to identify emerging research priorities in Indigenous cancer control.
Methods: A survey was administered to a network of individuals with an interest in cancer and Indigenous Australians. Respondents (N = 255) described what they thought was the most significant research priority for cancer control for Indigenous Australians and ranked prespecified research areas relating to components of the cancer continuum.
Results: Identified research priorities included cancer prevention and early detection; health literacy; and culturally appropriate care for Indigenous patients, survivors and families. Community engagement, Indigenous ownership, and partnership and collaboration were highlighted as critical elements underpinning research.
Conclusions: The identified research priorities, along with seminal documents such as the National Aboriginal and Torres Strait Islander Cancer Framework, provide a roadmap for developing, funding, implementing and translating research to reduce the burden of cancer for Indigenous Australians.
Full text
Introduction
Cancer is the second leading cause of death among Aboriginal and Torres Strait Islander people (respectfully referred to as Indigenous Australians), and is responsible for more deaths each year than diabetes and kidney disease combined.1 Indigenous Australians are more likely than other Australians to be diagnosed with rapidly fatal cancers (e.g. of the lung or liver) and less likely to be diagnosed with cancers that have better likelihood of survival (e.g. breast cancer or melanoma).2,3 In addition, many cancers that are amenable to prevention through reduced exposure to risk factors or early detection through screening programs are more common among Indigenous people.2-4 Among those diagnosed with cancer, Indigenous people are much less likely to survive than non-Indigenous people (5-year survival 40% compared with 52%, respectively).2
Despite the substantial impact of cancer on Indigenous people, its importance has only begun to be recognised. In 2010, a Cancer Australia–commissioned review of cancer and Indigenous people provided a comprehensive summary of evidence and included 31 recommendations for improving Indigenous cancer control, including service delivery, data infrastructure, prevention and programs.5 This was followed in late 2010 by the National Roundtable on Priorities for Aboriginal and Torres Strait Islander Cancer Research.6 A key directive from this roundtable was for a national, coordinated, collaborative, priority-driven, Indigenous-led research effort to improve Indigenous cancer outcomes.6 Subsequently, the National Health and Medical Research Council (NHMRC) funded a Centre for Research Excellence (CRE) in Discovering Indigenous Strategies to Improve Cancer Outcomes Via Engagement, Research Translation and Training (DISCOVER-TT), and Cancer Council NSW funded a 5-year Strategic Research Partnership grant (STREP Ca-CIndA), with supplemental funding from Cancer Council Western Australia, to improve cancer control for Indigenous Australians.
Several initiatives have arisen from the DISCOVER-TT/STREP Ca-CIndA research program, including the creation of the National Indigenous Cancer Network (NICaN)7; the development of the first National Aboriginal and Torres Strait Islander Cancer Framework, on behalf of and in conjunction with Cancer Australia8; and hosting the inaugural World Indigenous Cancer Conference (WICC) in 2016, in partnership with the International Agency for Research on Cancer.9 Other Australian initiatives include the development of an integrated cancer monitoring and surveillance system to improve cancer care for Aboriginal people in South Australia, which has anticipated relevance for other regions10; the use of social inclusion theory to improve cancer care11; and the assessment of patient navigator programs to improve diagnosis and treatment experiences.12
The capacity to monitor the health of Indigenous populations in Australia and other high-income countries is markedly hampered by the paucity of Indigenous identifiers in administrative datasets and cancer registries.13 However, evidence suggests that better health surveillance and targeted prevention, early detection, and vaccination programs are needed to reduce the higher rates of largely preventable cancers in Indigenous people in Australia, Canada, New Zealand and the US.13 In Canada, several studies have shown that cancer (of the cervix, colon and rectum, and breast) screening rates for Indigenous people are much lower than for non-Indigenous people.14-16 Research in New Zealand has looked at the role of cancer care in Indigenous cancer survival inequalities17, and called for the integration of cancer care across community-based cancer care, primary and secondary health care, and palliative care.18-20
The research landscape in Indigenous cancer control has changed substantially since landmark work in 2010, and it is timely to reassess the research agenda. In this paper, we present the results of a process, using an online survey of individuals with an interest in this area, to identify emerging research priorities and refine the research agenda for Indigenous cancer control in Australia.
Methods
Ethical approval was obtained from the Human Research Ethics Committee of the Northern Territory Department of Health and Menzies School of Health Research (HREC 2016-2671). An online survey with open- and closed-ended questions was developed, drawing on: 1) outcomes from the DISCOVER-TT/STREP Ca-CIndA research program, including annual research roundtables involving key stakeholders across Australia; 2) an environmental scan of international and national publicly available policies relating to cancer and Indigenous people; and 3) the WICC 2016 program. The recommendations and priorities identified from these sources (e.g. reports, publications, conference program themes) were synthesised to avoid repetition and categorised for inclusion in the survey into the following stages of the cancer continuum: prevention/early detection, diagnosis/treatment, supportive care/survivorship and palliative care.
The survey took approximately 15 minutes to complete, and asked participants to:
- Nominate and describe the most significant research priority (a significant research knowledge gap or unmet need) they felt needed to be addressed in the area of cancer and Indigenous Australians (open-ended response)
- Rank from predefined lists (prevention/early detection, diagnosis/treatment, supportive care/survivorship and palliative care) at least the top three research priorities within each list, with ‘1’ being the highest ranking. Respondents were also given an opportunity at the end of each list to add any relevant priorities that were not included in the list. However, this did not yield any new information beyond that reported elsewhere in the survey.
An email invitation to participate and a link to the survey were sent to the registered WICC mailing list (including all conference delegates) and the large network of people known to the DISCOVER-TT/STREP Ca-CIndA team (including NICaN members). The survey invitation was limited to people residing in Australia. Participants included researchers, public health practitioners, clinicians, nurses, advocacy groups, allied health and other related professionals, Indigenous cancer survivors and their families, and Indigenous community groups. Reminder emails were sent 2 and 3 weeks after the initial email. The survey closed after 4 weeks. As stated on the online survey cover page, participants provided informed consent by electing to take part in the survey.
Responses to open-ended questions were analysed using content analysis in NVivo qualitative data analysis software (QSR International version 11, 2015) and grouped into broad topic areas. The responses relating to each topic area were then reanalysed to gain a more nuanced interpretation of the topic as a research priority. Some priorities related to practice change or program implementation for improving service provision, which have been included here in recognition of the need to evaluate the efficacy and impact of a program. The ranked lists were assessed by calculating the percentage of respondents ranking an item as 1, 2 or 3, based on the total number of people who responded to that list. The synthesis of research priorities into a final list involved combining priorities that were common across both the qualitative responses and the top three ranked items from each section of the cancer continuum.
Results
Of 967 individuals and organisations invited to take part in the survey, 255 completed the survey (26% response rate). Of these respondents, 37% identified as being Aboriginal and/or Torres Strait Islander. Most respondents were female (79%) and aged between 45 and 54 years.
Most respondents lived in Queensland (30%) and New South Wales (25%); others lived in Victoria (15%), Western Australia (11%), South Australia (10%), the Northern Territory (7%), Tasmania (1%) and the Australian Capital Territory (1%). The majority lived in metropolitan areas (capital city or major cities with population >100 000 people: 71%); others lived in rural centres (population 10 000–100 000: 20%), and other rural/remote locations (population <10 000: 9%). Many respondents were in a health professional role (46%) and/or a carer/family member of someone affected by cancer (33%) (Figure 1). Among the health professionals, prominent roles included nurse (17%), Indigenous health worker (13%) and health promotion/preventive care/healthy lifestyles worker (12%).
Figure 1. Survey respondents’ role(s) or experience in cancer care (click to expand)
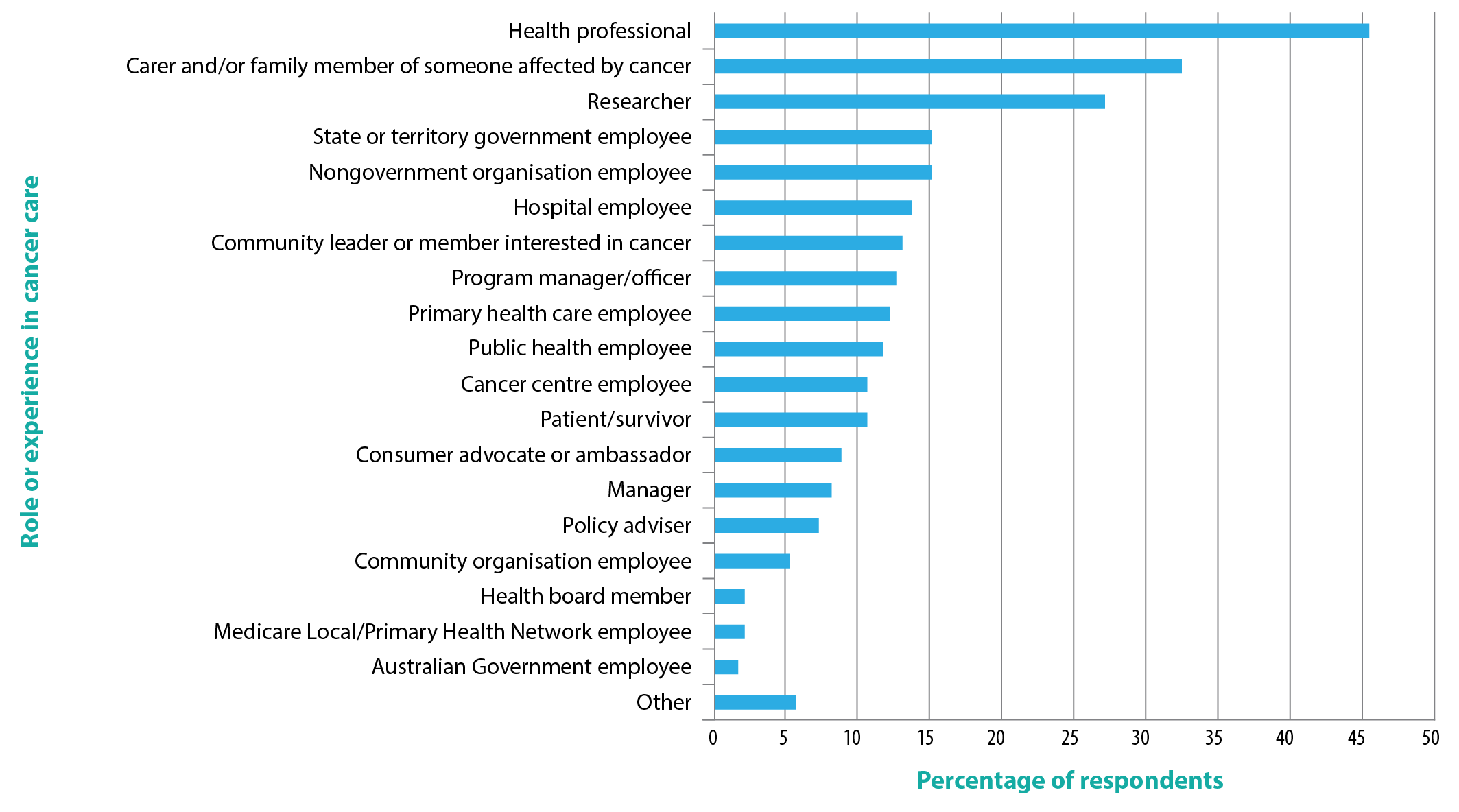
Note: Responses were not mutually exclusive.
Most respondents were working in, or interested in all aspects of, the cancer continuum (49%), followed by prevention (38%), treatment (33%), screening and early detection (32%), survivorship and living well after cancer (26%), diagnosis (23%), and palliative care (18%).
Research priorities identified in open-ended questions
Content analysis of open-ended responses revealed that the 10 most commonly reported priorities could be grouped into the following three categories: cancer prevention and early detection, patient engagement with the system, and system-wide factors.
Cancer prevention and early detection
Prevention and healthy lifestyles
Cancer prevention was commonly cited as the most significant priority, with a focus on diet, smoking, alcohol and exercise. Social determinants of cancer were commonly cited, including intergenerational trauma and socio-economic disadvantage. Respondents reported that prevention strategies should target specific communities, use a lifecourse approach, involve community consultation and focus on primary health care.
Community education and health promotion
Many respondents called for research focusing on screening-related community education programs, community awareness about the link between lifestyle and cancer, and raising awareness of the benefits of early detection. An unwillingness to talk about cancer in Indigenous communities, together with shame and stigma associated with a cancer diagnosis, were identified as key issues. Respondents reported that education initiatives should be culturally appropriate, target youth and empower Indigenous communities.
Cancer screening
Screening was commonly reported as the foundation for reducing Indigenous cancer mortality. Improving data on Indigenous participation rates in screening programs was flagged, as was targeting underscreened and never-screened groups. Understanding the barriers to accessing and engaging in screening, and developing more proactive approaches were commonly cited, including outreach programs, community-based events, general health check-ups, and training for general practitioners and Indigenous health workers.
Timely diagnosis and early detection
The issue of timely diagnosis permeated respondents’ comments across priorities and was identified as a critical goal of many other research priorities.
Engaging with the health system
Experience of care and system navigation
The inclusion of the views and experiences of Indigenous patients, families and the community in cancer research was commonly called for – specifically, approaches that are participatory, transformational and lead to rapid improvements in patient outcomes. Respondents identified the need to better understand patients’ experiences of care, supportive requirements and cultural preferences to better facilitate patient-centred care.
Engagement with, and access to, services
Understanding the barriers and facilitators to Indigenous Australians’ engagement with, and access to, health services was called for to improve screening rates, treatment efficacy and cancer outcomes. Issues identified as requiring research included health literacy, remote location, socio-economic disadvantage, cultural safety, language difference, impersonal approaches and fear.
Culturally appropriate services and educational materials
Respondents described the importance of developing culturally aware and responsive cancer services based on the needs, expectations and preferences of Indigenous patients. Systemic racism and poor understanding of Indigenous peoples’ history and culture were highlighted as impediments to fostering culturally appropriate care.
System-wide factors
Indigenous workforce
Increasing the number of Indigenous people working in all areas of the health system was widely mentioned. The need to improve support, education and opportunities for Indigenous people in the health workforce was identified as key to creating culturally appropriate services, and fostering effective and positive engagement with patients.
Remote community issues
The compounding disadvantages experienced by Indigenous Australians in remote areas was interwoven throughout the respondents’ comments. The pressing need for high-quality cancer services in regional and remote areas was made clear, including increased cancer-specific training for remote health providers, greater incentives to retain local staff, greater coverage of cancer outreach services, and improved access to technology and diagnostic facilities. Several respondents reported that Indigenous Australians living in remote areas face substantive barriers to engaging with urban-based cancer services, including financial and logistical difficulties of travel, accommodation and childcare; cultural and language differences; lack of family and community support; and a widespread lack of understanding of these challenges by non-Indigenous care providers. Researching the challenges facing remote Indigenous peoples with cancer was described as important in achieving equity in access to care.
Community engagement and self-determination
Increasing Indigenous involvement and data sovereignty in cancer research was described as critical to ensuring that Indigenous values and priorities underpin research. A greater focus on community education, face-to-face consultation and inclusion of community members in clinical, policy and research leadership were identified as essential steps towards servicing the needs of Indigenous Australians more effectively and in reducing cancer disparity.
Ranked research priorities across the cancer continuum
Respondents’ rankings on the four prespecified lists were largely consistent with the open-ended responses relating to research priorities. Research priorities are presented in ranked order for each list in Table 1a–d.
Table 1. Ranked research priorities for Indigenous cancer control across the cancer continuum
a Prevention and early detection (n = 182)
| Rank | Priority | n | %a |
| 1 | Develop and evaluate programs that increase awareness and understanding of preventable cancer risks (e.g. tobacco smoking, unhealthy weight, hazardous alcohol consumption, sedentary lifestyle, poor nutrition) | 79 | 43.4 |
| 2 | Identify the barriers and enablers to participation in cancer screening for Indigenous people | 60 | 33.0 |
| 3 | Identify ways to improve cancer health literacy in the workforce and community | 56 | 30.8 |
| 4 | Identify how to overcome these barriers and increase screening rates through culturally appropriate outreach efforts | 54 | 29.7 |
| 5 | Identify the best ways to improve Indigenous people’s awareness of early signs and symptoms of cancers | 52 | 28.6 |
| 5 | Identify specific barriers and enablers to minimise cancer risk for Indigenous people | 52 | 28.6 |
| 6 | Identify ways that the health workforce can engage communities in early screening and detection initiatives | 36 | 19.8 |
| 7 | Understand stigma and shame regarding cancer and screening for cancer, and ways to overcome this | 30 | 16.5 |
| 8 | Identify the best ways to follow up on early signs and symptoms of cancers | 28 | 15.4 |
| 9 | Identify best-practice models of delivery of cancer screening programs | 25 | 13.7 |
| 10 | Research hereditary links, change of diet, environmental pollutants, and their impact on cancer rates in Indigenous people | 22 | 12.1 |
| 11 | Improve knowledge/understanding of known environmental risk factors | 14 | 7.7 |
| 12 | Find local explanations for why particular cancers are of concern in particular areas | 13 | 7.1 |
| 13 | Identify barriers and enablers to maximise vaccination uptake | 9 | 5.0 |
a Percentage of respondents who ranked the item as 1, 2 or 3.
b Diagnosis and treatment (n = 167)
| Rank | Priority | n | %a |
| 1 | Identify new models of care to meet the needs of rural and remote Indigenous communities, to improve access to programs and services | 89 | 53.3 |
| 1 | Identify how to improve the acceptability and accessibility of health services and their responsiveness to the needs of Indigenous people | 89 | 53.3 |
| 2 | Develop, implement and evaluate culturally responsive resources | 59 | 35.3 |
| 3 | Develop, implement and evaluate culturally appropriate patient navigation | 53 | 31.7 |
| 4 | Identify the best approaches to facilitate and sustain Indigenous ownership and involvement in all aspects of service delivery | 52 | 31.1 |
| 5 | Identify new models of care to meet the needs of Indigenous people in metropolitan areas, to improve access to programs and services | 47 | 28.1 |
| 6 | Understand the impact of complex health needs, including high rates of comorbidities | 38 | 22.8 |
| 7 | Assess ways to improve capacity to identify Indigenous cancer patients correctly | 23 | 13.8 |
| 8 | Identify optimal ways to assess and manage supportive care needs | 22 | 13.2 |
| 9 | Improve measurement of patient experience and outcomes | 21 | 12.6 |
| 10 | Identify optimal ways to assess and manage clinical needs | 17 | 10.2 |
a Percentage of respondents who ranked the item as 1, 2 or 3.
c Supportive care and survivorship (n = 165)
| Rank | Priority | n | %a |
| 1 | Identify physical, mental, spiritual, practical and financial needs of patients and their families, and ensure access to programs and services that address these needs | 114 | 69.1 |
| 2 | Identify optimal ways to provide supportive care beyond treatment completion | 83 | 50.3 |
| 3 | Develop greater understanding of the needs of other people involved in an Indigenous patient’s cancer journey (e.g. carers) | 65 | 39.4 |
| 4 | Develop, implement and evaluate patient navigation programs for cancer survivors | 63 | 38.2 |
| 5 | Pilot innovative transition services for patients with cancer between cancer care centres and home | 60 | 36.4 |
| 6 | Understand ways to involve and inform families and carers of Indigenous people with cancer | 49 | 29.7 |
| 7 | Understand ways in which peer support can help Indigenous cancer survivors | 41 | 24.9 |
a Percentage of respondents who ranked the item as 1, 2 or 3.
d Palliative care (n = 159)
| Rank | Priority | n | %a |
| 1 | Increase understanding of, and address barriers to, access and use of palliative care services by Indigenous people | 123 | 77.4 |
| 2 | Identify best ways to deliver culturally appropriate palliative care | 116 | 73.0 |
| 2 | Identify the palliative care needs of Indigenous cancer patients and their families | 116 | 73.0 |
| 3 | Develop and evaluate training models for clinicians to be trained in end-of-life care and palliation | 54 | 34.0 |
| 4 | Identify effective referral pathways for palliative care | 51 | 32.1 |
a Percentage of respondents who ranked the item as 1, 2 or 3.
Synthesised list of research priorities
The key research priority areas for improving cancer control for Indigenous Australians are summarised in Box 1.
Box 1. Summary of research priorities for improving cancer control for Indigenous Australians
Cancer prevention and early detection
- Develop and evaluate ways to increase awareness and understanding of cancer risks, symptoms and cancer screening
- Understand the barriers and enablers to participation in cancer screening programs
- Develop, implement and evaluate evidence based strategies to increase participation in cancer screening
Health literacy
- Identify ways to improve cancer health literacy in the health workforce and community
- Develop, implement and evaluate culturally responsive resources
Culturally appropriate care for cancer survivors and their carers/family
- Implement and evaluate culturally appropriate outreach efforts and health services (at a system-wide level rather than individual services)
- Identify new models of care for Indigenous people in rural, remote and metropolitan areas
- Assess the acceptability and accessibility of health services and their responsiveness to needs
- Identify barriers and enablers to accessing and completing treatment
- Identify unmet needs (e.g. physical, spiritual, financial, practical) and ensure that programs and services are in place to meet those needs
- Develop, implement and evaluate patient navigation programs
- Investigate ways to improve survivorship care (i.e. beyond treatment completion)
- Identify the needs of carers and develop ways to support the family
- Understand palliative care needs and identify barriers to accessing palliative services for families and patients
Cross-cutting themes
- The need to establish partnerships and to collaborate with key stakeholders
- Community engagement and Indigenous ownership in all aspects of the research process
Discussion
The research priority areas identified in this project advocate focus in the areas of cancer prevention and early detection; health literacy; and provision of culturally appropriate care for patients, survivors and families. Underpinning this research are critical elements of meaningful community engagement, Indigenous ownership, and working in partnership and collaboration to reduce the burden of cancer on Indigenous Australians. We recognise that some priorities relate to changes that could be made in the short term based on existing knowledge. However, these are included as research priorities in recognition of the importance of evaluating the barriers and facilitators to successful implementation, and assessing the effectiveness and impact of such changes in real-world settings.
The priorities identified in this project are broadly consistent with the priority areas for action in the National Aboriginal and Torres Strait Islander Cancer Framework.8 The identified research priorities are particularly consistent with framework priorities 1 (improving knowledge, attitudes and understanding), 5 (optimal and culturally appropriate treatment, support and care) and 7 (strengthening capacity of health services). The results of this project provide a way forward for “targeted and priority research to inform policy, health promotion, service provision and practice” (framework priority 7b).
As was the case with the development of the Framework, the research priorities identified in this project were developed through the involvement of key stakeholders, including a broad range of researchers, public health practitioners, clinicians, nurses, advocacy groups, allied health and other related professionals, Indigenous cancer survivors and their families, and Indigenous community groups. These comprehensive findings represent a broad consensus of key people involved in cancer control for Indigenous people.
As a result of the recent increase in attention on Indigenous cancer control, there is now greater awareness among policy makers, health service providers, and Indigenous leaders and communities, as well as a more active research effort across several research groups. However, much research remains to be done across the cancer continuum to improve cancer outcomes for Indigenous Australians.
Limitations of the project include the low response rate (26%) and the inability to determine whether the respondents were representative of the larger database of people invited to participate, because of the lack of demographic information in the database. However, a significant proportion of the respondents identified as Indigenous, were geographically diverse, and represented a variety of occupations and consumer groups.
The identified list of current research priorities, along with seminal documents such as the National Aboriginal and Torres Strait Islander Cancer Framework8, provide a useful roadmap to guide the development, funding, implementation and translation of research and service development to reduce the burden of cancer for Indigenous Australians. This roadmap can be used by researchers, policy makers and service providers to focus on key areas to improve cancer control for Indigenous people. Funding bodies can also use the priority actions from the framework and the priority research areas identified in this project to focus future research.
Acknowledgements
This project was undertaken under the auspices of the DISCOVER-TT CRE (funded by the NHMRC, 1041111) and the STREP Ca-CIndA (funded through Cancer Council NSW (SRP 13-01), with supplementary funding from Cancer Council Western Australia. We also acknowledge the ongoing support of the Lowitja Institute, Australia’s National Institute for Aboriginal and Torres Strait Islander Health Research. JC was supported by an NHMRC Research Fellowship (1058244). GG was supported by an NHMRC Early Career Fellowship (1105399). The views expressed in this publication are those of the authors and do not necessarily reflect the views of the funding agencies.
Copyright:

© 2017 Morris et al. This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence, which allows others to redistribute, adapt and share this work non-commercially provided they attribute the work and any adapted version of it is distributed under the same Creative Commons licence terms.
References
- 1. Australian Institute of Health and Welfare. The health and welfare of Australia’s Aboriginal and Torres Strait Islander peoples 2015. Canberra: AIHW; 2015 [cited 2017 Aug 20]. Available from: www.aihw.gov.au/getmedia/584073f7-041e-4818-9419-39f5a060b1aa/18175.pdf.aspx?inline=true
- 2. Australian Institute of Health and Welfare, Cancer Australia. Cancer in Aboriginal and Torres Strait Islander peoples of Australia: an overview. Canberra: AIHW; 2013 [cited 2017 Aug 20]. Available from: trove.nla.gov.au/work/186996677?q&versionId=204496678
- 3. Cunningham J, Rumbold AR, Zhang X, Condon JR. Incidence, aetiology and outcomes of cancer in Indigenous peoples in Australia. Lancet Oncol. 2008;9(6):585–95. CrossRef | PubMed
- 4. Australian Institute of Health and Welfare. Cancer in Australia 2017. Canberra: AIHW; 2017 [cited 2017 Aug 20]. Available from: www.aihw.gov.au/getmedia/3da1f3c2-30f0-4475-8aed-1f19f8e16d48/20066-cancer-2017.pdf.aspx?inline=true
- 5. Miller J, Knott V, Wilson C, Cunningham J, Condon J, Roder D, et al. Aboriginal and Torres Strait Islander cancer control research project. Sydney: Cancer Australia; 2010 [cited 2017 Aug 20]. Available from: canceraustralia.gov.au/system/tdf/publications/atsi_cancer_control_research_report1_504af02522aa1.pdf?file=1&type=node&id=2836
- 6. Garvey G, Cunningham J, Valery PC, Condon J, Roder D, Bailie R, et al. Reducing the burden of cancer for Aboriginal and Torres Strait Islander Australians: time for a coordinated, collaborative, priority-driven, Indigenous-led research program. Med J Aust. 2011;194(10):530–1. PubMed
- 7. National Indigenous Cancer Network. Brisbane: NICaN [cited 2017 Aug 20]. Available from: www.nican.org.au
- 8. Cancer Australia. National Aboriginal and Torres Strait Islander cancer framework. Sydney: Cancer Australia; 2015 [cited 2017 Aug 23]. Available from: canceraustralia.gov.au/sites/default/files/publications/national-aboriginal-and-torres-strait-islander-cancer-framework/pdf/2015_atsi_framework_1.pdf
- 9. World Indigenous Cancer Conference Network. Brisbane: WICC Network [cited 2017 Aug 23]. Available from: www.wiccnetwork.org
- 10. Yerrell PH, Roder D, Cargo M, Reilly R, Banham D, Micklem JM, et al. Cancer data and Aboriginal disparities (CanDAD)—developing an advanced cancer data system for Aboriginal people in South Australia: a mixed methods research protocol. BMJ Open. 2016;6:e012505. CrossRef | PubMed
- 11. Treloar C, Gray R, Brener L, Jackson C, Saunders V, Johnson P, et al. “I can’t do this, it’s too much”: building social inclusion in cancer diagnosis and treatment experiences of Aboriginal people, their carers and health workers. Int J Public Health. 2014;59(2):373–9. CrossRef | PubMed
- 12. Bernardes CM, Martin J, Cole P, Kitchener G, Cowburn G, Garvey G, et al. Lessons learned from a pilot study of an Indigenous patient navigator intervention in Queensland, Australia. Eur J Cancer Care. 2017:e12714. CrossRef | PubMed
- 13. Moore SP, Antoni S, Colquhoun A, Healy B, Ellison-Loschmann L, Potter JD, et al. Cancer incidence in indigenous people in Australia, New Zealand, Canada, and the USA: a comparative population-based study. Lancet Oncol. 2015;16:1483–92. CrossRef | PubMed
- 14. Decker KM, Demers AA, Kliewer EV, Biswanger N, Musto G, Elias B, et al. Pap test use and cervical cancer incidence in First Nations women living in Manitoba. Cancer Prev Res. 2015;8(1):49–55. CrossRef | PubMed
- 15. Decker KM, Demers AA, Kliewer EV, Musto G, Shu E, Biswanger N, et al. Colorectal cancer screening in First Nations people living in Manitoba. Cancer Epidemiol Biomarkers Prev. 2015;24(1):241–8. CrossRef | PubMed
- 16. Demers AA, Decker KM, Kliewer EV, Musto G, Shu E, Biswanger N, et al. Mammography rates for breast cancer screening: a comparison of First Nations women and all other women living in Manitoba, Canada, 1999–2008. Prev Chronic Dis. 2015;12:E82. CrossRef | PubMed
- 17. Hill S, Sarfati D, Robson B, Blakely T. Indigenous inequalities in cancer: what role for health care? ANZ J Surg. 2013;83(1–2):36–41. CrossRef | PubMed
- 18. Robson B, Ellison-Loschmann L. Maori and cancer care in Aotearoa/New Zealand – responses to disparities. Eur J Cancer Care. 2016;25(2):214–8. CrossRef | PubMed
- 19. Slater T, Matheson A, Davies C, Goodyer C, Holdaway M, Ellison-Loschmann L. The role and potential of community-based cancer care for Māori in Aotearoa/New Zealand. N Z Med J. 2016;129(1430):29–38. PubMed
- 20. Slater T, Matheson A, Davies C, Tavite H, Ruhe T, Holdaway M, Ellison-Loschmann L. ‘It’s whanaungatanga and all that kind of stuff’: Maori cancer patients’ experiences of health services. J Prim Health Care. 2013;5(4):308–14. PubMed